 Back
BackAcid-Fast Bacilli and Gram-Negative Rods of Medical Importance: Mycobacteria, Bordetella, and Pasteurellaceae
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Mycobacteria: Acid-Fast Bacilli
Acid-Fast Staining and Cell Wall Structure
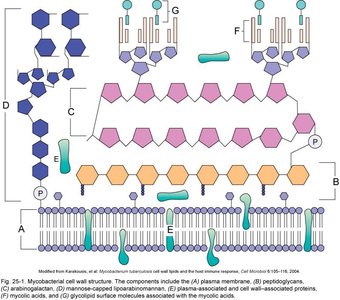
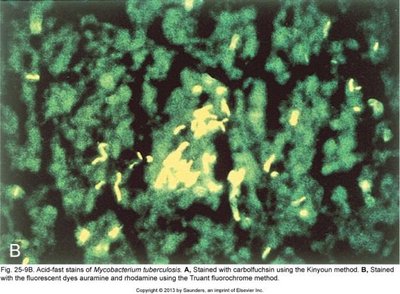
Mycobacteria are a unique group of bacteria characterized by their acid-fastness, which is due to the presence of mycolic acids in their cell wall. These organisms are Gram-positive with a distinctive cell wall structure that lacks an outer membrane but contains a thick peptidoglycan layer and various complex lipids.
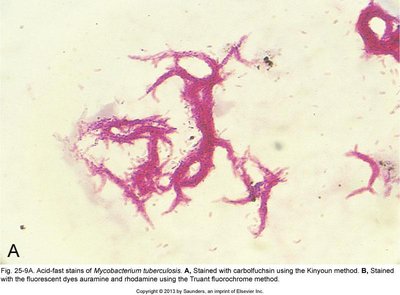
Acid-fast staining: A differential staining technique used to identify mycobacteria, which retain the primary stain even after acid-alcohol decolorization due to their lipid-rich cell wall.
Cell wall composition: Contains mycolic acids, phosphatidylinositol mannosides, lipoarabinomannan, additional lipids, glycolipids, peptidoglycolipids, and various proteins (often antigenic).
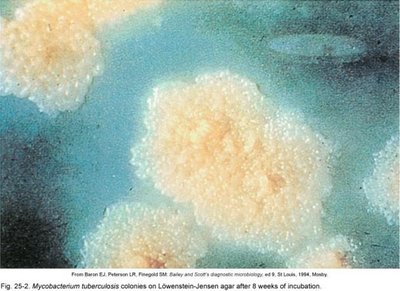
Growth characteristics: Strict aerobes, catalase positive, non-motile, non-encapsulated, and many species are slow-growing.
Diversity: Over 150 species identified.
Classification of Mycobacteria
Mycobacteria are classified based on growth rate, pigmentation, and pathogenicity:
Mycobacterium tuberculosis complex: Slow-growing, non-pigmented, not all cause tuberculosis.
Slow-growing nontuberculous mycobacteria: Often pigmented.
Rapidly growing nontuberculous mycobacteria: Grow faster than the above groups.
Mycobacterium tuberculosis: Pathogenesis and Disease
Mycobacterium tuberculosis is the causative agent of tuberculosis (TB), a major infectious disease worldwide. Infection occurs via inhalation of a low infectious dose, and the bacteria are phagocytosed by macrophages, where they block phagosome-lysosome fusion.
Immune response: Macrophages release IL-12 and TNF, recruiting NK and T cells, which produce IFN-γ to activate macrophages.
Granuloma formation: After 3-4 weeks, tubercles (granulomas) form, which may heal by calcification or break down into necrotic caseous lesions.
Latent and active TB: Small tubercles may clear infection; large ones protect bacteria. Reactivation (secondary TB) is more likely in immunosuppressed individuals.
Symptoms of active TB: Violent coughing, greenish/brown or bloody sputum, fever, anorexia, fatigue. Untreated, mortality can reach 60%.
Extrapulmonary TB: Bacilli may spread to lymph nodes, kidneys, bones, genital tract, or brain, especially in immunocompromised patients.
Diagnosis of Tuberculosis
Diagnosis involves a combination of clinical, radiological, and laboratory methods:
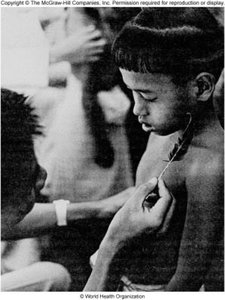
In vivo tuberculin testing (Mantoux test): Intradermal injection of purified protein derivative (PPD); a red wheal indicates a T cell response within 48-72 hours.
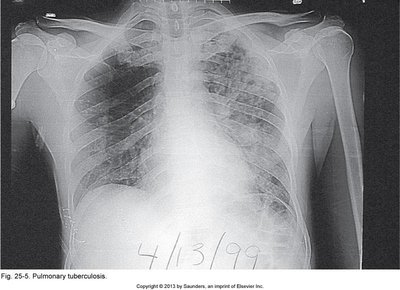
Chest X-rays: Used to detect pulmonary involvement.
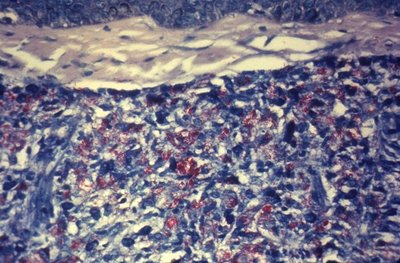
Acid-fast bacilli in specimens: Microscopy of sputum or tissue samples.
Culture and biochemical testing: Growth on specialized media and identification by biochemical assays.
Newer tests: Blood tests for IFN-γ production (e.g., QuantiFERON-TB Gold) are more accurate and can distinguish M. tuberculosis from other mycobacteria.

Management and Prevention of Tuberculosis
Treatment of TB requires prolonged multidrug therapy due to the slow growth and resistance potential of mycobacteria.
Standard regimen: 6-24 months of at least two drugs (e.g., isoniazid, rifampin, ethambutol, pyrazinamide).
Drug resistance: Multidrug-resistant (MDR) and extensively drug-resistant (XDR) TB are significant challenges.
Prevention: Prophylaxis for exposed individuals, BCG vaccine (variable efficacy), and public health measures.
Mycobacterium leprae and M. lepromatosis: The Leprosy Bacilli
Overview and Pathogenesis
Leprosy (Hansen’s Disease) is caused by Mycobacterium leprae and M. lepromatosis. These are strict parasites that multiply in host cells and have not been cultured outside living hosts.
Transmission: Prolonged droplet contact over months; not highly virulent.
Incubation: 2-10 years; nerve damage is a hallmark.
Major forms: Tuberculoid (localized, TH1 response, nerve damage) and Lepromatous (disseminated, TH2 response, severe disfigurement).
WHO classification: Paucibacillary (<5 lesions) vs. multibacillary.




Diagnosis and Treatment of Leprosy
Diagnosis: Based on clinical findings (skin lesions, nerve involvement), acid-fast bacilli in lesions or nasal discharge, and patient history.
Treatment: Combination therapy with dapsone, rifampin, and clofazimine for 6-12 months or longer depending on disease form.
Prevention: Early detection, prophylaxis of contacts, isolation, and vaccination (BCG may offer some protection).
Other Mycobacteria of Medical Importance
Mycobacterium avium Complex (MAC)
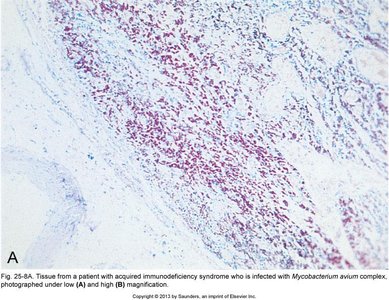
MAC includes M. avium and M. intracellulare, which can cause chronic pulmonary disease in immunocompetent individuals and disseminated disease in immunocompromised patients (especially AIDS).
Risk groups: Older men, smokers, people with respiratory problems, and immunocompromised individuals.
Clinical syndromes: Chronic pulmonary disease, "Lady Windermere syndrome," and disseminated multiorgan infection.
Other Slow and Fast-Growing Mycobacteria
Slow-growing: M. bovis, M. kansasii (pulmonary), M. scrofulaceum (lymphatics, scrofula), M. ulcerans (Buruli ulcer), M. marinum (swimming pool granuloma), M. haemophilum.
Fast-growing: M. fortuitum, M. chelonae, M. abscessus, M. mucogenicum (skin infections, often after trauma or medical procedures).
Diagnosis of Mycobacterial Infections
Microscopy: Acid-fast staining of specimens.
Culture: Assessment of pigmentation, growth rate, temperature, and hemin requirements.
Nucleic acid tests: PCR and specific probes for rapid identification and sensitivity testing.
Gram-Negative Rods of Medical Importance
Bordetella pertussis (Whooping Cough)
Bordetella pertussis is a tiny, encapsulated Gram-negative coccobacillus that causes pertussis (whooping cough), a highly contagious acute respiratory syndrome.
Transmission: Direct contact or inhalation of aerosols from healthy carriers.
Virulence factors: Adhesins (filamentous hemagglutinin, pertactin, fimbriae), pertussis toxin (increases cAMP), adenylate cyclase/hemolysin, dermonecrotic toxin, tracheal cytotoxin.
Disease stages: Catarrhal (cold-like, most infectious), paroxysmal (severe coughing), convalescent (recovery, possible complications).
Complications: Pneumonia, seizures, encephalopathy, apnea, and death (especially in infants).

Diagnosis and Prevention of Pertussis
Diagnosis: Culture (difficult), antibody tests, PCR (most sensitive), detection of antibodies to pertussis toxin.
Treatment: Antibiotics (macrolides) for prophylaxis; treatment often started late due to delayed diagnosis.
Prevention: DTaP vaccine for children, Tdap for adults and pregnant women.
Pasteurellaceae Family
General Characteristics
The Pasteurellaceae are small, Gram-negative rods that are facultative anaerobes and often require enriched media for growth. Important genera include Haemophilus, Actinobacillus, Aggregatibacter, and Pasteurella.
Haemophilus Species
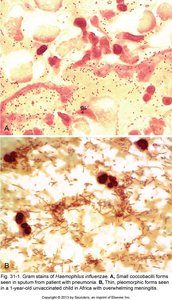
General features: Oxidase positive, pleomorphic rods, very fastidious (require chocolate agar), sensitive to drying and disinfectants.
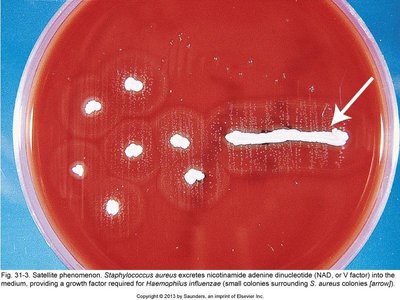
Sattelitism: Growth around colonies of other bacteria (e.g., Staphylococcus aureus) that provide necessary growth factors.
Normal flora: Some species are part of the normal respiratory or vaginal flora.
Haemophilus influenzae
Capsule: Six serotypes; serotype b (Hib) was most important before vaccination.
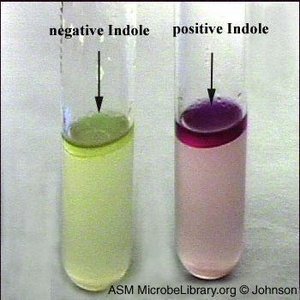
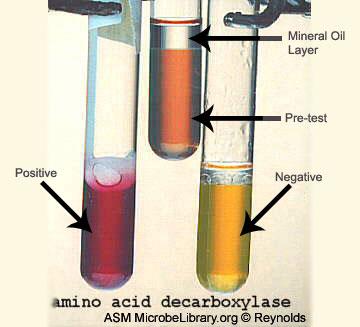
Biotypes: Identified by biochemical assays (indole, urease, ornithine decarboxylase activity).
Virulence factors: Pili, adhesins, IgA protease, endotoxin.
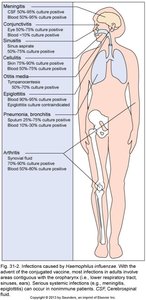
Diseases: Meningitis, epiglottitis, cellulitis (capsulated strains); otitis media, sinusitis, and pneumonia (non-capsulated strains).
Control: Hib vaccine is highly effective; cephalosporins for severe infections.
Other Haemophilus Species
H. aegyptius: Causes conjunctivitis ("pink eye"), can cause Brazilian purpuric fever (high mortality).
H. ducreyi: Causes chancroid (STI with soft, painful chancres); treated with macrolides or cephalosporins.
H. parainfluenzae and H. aphrophilus: Normal oral flora; can cause dental abscesses and infective endocarditis.
Other Pasteurellaceae
Actinobacillus: Normal flora in animals and humans; rare opportunistic infections (bites, pneumonia).
Aggregatibacter: Oral flora; can cause subacute endocarditis.
Pasteurella: Found in the oropharynx of animals; causes cellulitis after bites, scratches, or licks (especially P. multocida).
