 Back
BackAntimicrobial Drugs: Mechanisms, Classes, and Resistance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Antimicrobial Drugs: Introduction and Historical Perspective
Discovery and Impact
Antimicrobial drugs are compounds used to kill or inhibit the growth of microbes, revolutionizing modern medicine by drastically reducing mortality from infectious diseases. They are classified based on the type of pathogen they target: antibacterial, antiviral, antifungal, and antiparasitic drugs.
Alexander Fleming discovered penicillin in 1928 while studying Staphylococcus aureus. He observed that a mold, later identified as Penicillium, inhibited bacterial growth.
Streptomycin, isolated from Streptomyces griseus, was the first antibiotic effective against tuberculosis.

Classification and Mechanisms of Antimicrobial Drugs
Spectrum of Activity
Broad-spectrum drugs: Effective against a wide range of Gram-positive and Gram-negative bacteria. Used in empiric therapy when the pathogen is unknown.
Narrow-spectrum drugs: Target a limited range of bacteria, minimizing disruption to normal microbiota. Preferred when the pathogen is identified.
Bacteriostatic vs. Bactericidal
Bacteriostatic drugs: Inhibit bacterial growth, often by targeting protein synthesis or metabolic pathways.
Bactericidal drugs: Kill bacteria, typically by targeting cell walls, membranes, or nucleic acids.
The distinction can depend on pathogen type, drug dose, regimen length, and administration route.
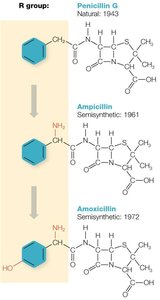
Natural, Semisynthetic, and Synthetic Antimicrobials
Antibiotics: Naturally occurring antimicrobial compounds (e.g., penicillin).
Synthetic antimicrobials: Fully manufactured by chemical processes (e.g., fluoroquinolones).
Semisynthetic antimicrobials: Chemically modified natural antibiotics to enhance properties (e.g., ampicillin, amoxicillin).
Key Pharmacological Concepts
Therapeutic index: Ratio of maximum tolerated dose to minimum effective dose. High index = safer drug. Equation:
Selective toxicity: Drug targets microbial structures/processes not found in human cells.
Half-life: Time for half the drug dose to be eliminated from the body. Determines dosing frequency.
Hepatotoxicity (liver damage) and nephrotoxicity (kidney damage) are important side effects to monitor.
Survey of Antibacterial Drugs
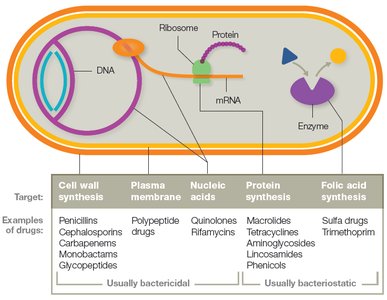
Cellular Targets and Drug Families
Antibacterial drugs are grouped by their cellular targets and mechanisms of action.
Target | Drug Family | Examples | Activity Spectrum |
|---|---|---|---|
Cell wall synthesis | Penicillins, Cephalosporins, Carbapenems, Monobactams, Glycopeptides | Penicillin G, Cephalexin, Imipenem, Aztreonam, Vancomycin | Narrow to broad |
Plasma membrane | Polypeptide drugs | Polymyxin B, Colistin | Narrow |
Nucleic acids | Quinolones, Rifamycins | Ciprofloxacin, Rifampin | Broad |
Protein synthesis (ribosomes) | Macrolides, Lincosamides, Phenicols, Tetracyclines, Aminoglycosides | Erythromycin, Clindamycin, Chloramphenicol, Doxycycline, Gentamicin | Broad or narrow |
Folic acid synthesis | Sulfa drugs, Trimethoprim | Sulfamethoxazole, Trimethoprim | Broad |
Cell Wall Synthesis Inhibitors
Most bacteria have a peptidoglycan cell wall. Drugs like penicillins block transpeptidation, weakening the wall and causing cell lysis.

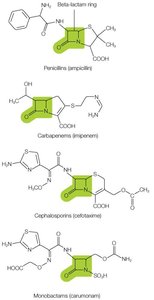
Beta-Lactam Drugs
All contain a beta-lactam ring and inhibit transpeptidase enzymes.
Families: Penicillins, Cephalosporins, Carbapenems, Monobactams.
Beta-lactamases are bacterial enzymes that inactivate these drugs; beta-lactamase inhibitors (e.g., clavulanate) are used in combination therapies.
Penicillins
Natural (Penicillin G, Penicillin V) and semisynthetic (ampicillin, amoxicillin) forms exist.
Some penicillins are modified to resist beta-lactamases (e.g., methicillin, oxacillin).
Common side effects: rashes, GI upset; allergies are a concern.
Cephalosporins
Five generations, with increasing Gram-negative activity and decreasing Gram-positive activity.
Fifth-generation (e.g., ceftaroline) effective against MRSA/ORSA.
Carbapenems and Monobactams
Carbapenems: Broad spectrum, reserved for multidrug-resistant infections.
Monobactams (e.g., aztreonam): Narrow spectrum, effective against Gram-negative bacteria.
Glycopeptides
Non-beta-lactam drugs (e.g., vancomycin, teicoplanin) that inhibit cell wall synthesis.
Effective against Gram-positive bacteria, including MRSA; not absorbed orally except for intestinal infections.
Side effects: "Red man syndrome," taste disturbances, nausea.

Other Cell Wall Inhibitors
Bacitracin: Topical use, effective against Gram-positive bacteria.
Isoniazid: Used for tuberculosis, inhibits mycolic acid synthesis in acid-fast bacteria.
Drugs Targeting Nucleic Acids
Quinolones (e.g., ciprofloxacin, levofloxacin): Inhibit DNA gyrase and topoisomerases; broad spectrum; reserved for resistant infections.
Rifamycins (e.g., rifampin): Inhibit RNA polymerase; effective against mycobacteria; significant drug interactions.
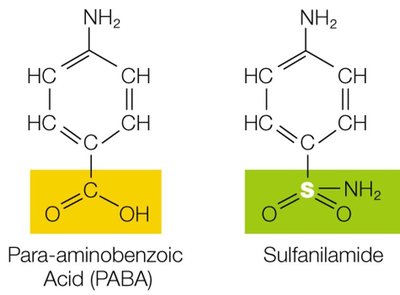
Drugs Targeting Folic Acid Synthesis
Sulfa drugs (sulfonamides): Competitive inhibitors of folic acid synthesis; bacteriostatic; broad spectrum.
Do not affect human cells, which do not synthesize folic acid.

Common side effects: rash, GI upset, photosensitivity; frequent allergies.
Used topically (e.g., silver sulfadiazine for burns) and systemically.

Drugs Targeting Prokaryotic Ribosomes (Protein Synthesis Inhibitors)
Bind to 50S or 30S ribosomal subunits, inhibiting protein synthesis (often bacteriostatic).
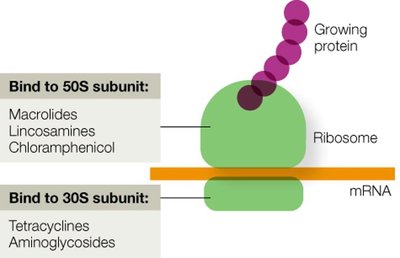
Macrolides (e.g., erythromycin, azithromycin): Broad spectrum; treat respiratory, skin, and soft tissue infections.
Lincosamides (e.g., clindamycin): Broad spectrum; effective against MRSA; risk of C. difficile colitis.
Phenicols (e.g., chloramphenicol): Broad spectrum; reserved for severe infections due to toxicity (bone marrow suppression).
Tetracyclines (e.g., doxycycline): Broad spectrum; not for children under 8 due to effects on teeth and bones; photosensitivity risk.
Aminoglycosides (e.g., gentamicin, streptomycin): Narrow spectrum (Gram-negative); risk of nephrotoxicity and hearing loss; often used in combination therapy.
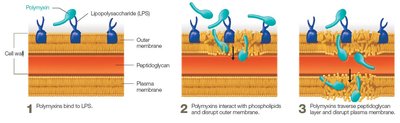
Drugs Targeting Cell Membranes
Polypeptide drugs (e.g., polymyxin B, colistin): Disrupt Gram-negative outer and plasma membranes; narrow therapeutic index; used topically or for multidrug-resistant infections.
Antimicrobial Drugs Against Viruses, Fungi, Protozoa, and Helminths
Antiviral Drugs
Target specific stages of viral replication: attachment, penetration, uncoating, replication/assembly, release.
Most effective against actively replicating viruses; latent viruses are difficult to treat.
Antifungal Drugs
Target fungal cell wall (e.g., echinocandins), plasma membrane (e.g., azoles, allylamines, polyenes), or nucleic acid synthesis (e.g., flucytosine).
Polyenes (e.g., amphotericin B, nystatin) interact with ergosterol, causing membrane leakage; nephrotoxicity is a concern.
Antiprotozoan and Antihelminthic Drugs
Antimalarial drugs: Aminoquinolines, artemisinins, and others target Plasmodium species.
Nonmalarial antiprotozoan drugs: Metronidazole, TMP/SMX, nitazoxanide.
Antihelminthic drugs: Albendazole, mebendazole (inhibit glucose uptake); praziquantel (paralyzes worms).
Assessing Sensitivity to Antimicrobial Drugs
Antibiotic Susceptibility Testing
Essential for guiding therapy and combating resistance.
Common methods: Kirby-Bauer disk diffusion, E-test, broth dilution tests.
Kirby-Bauer Test
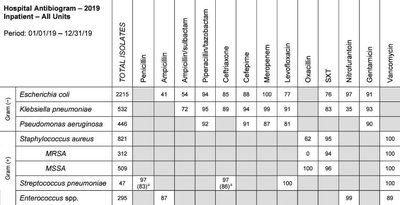
Bacteria are spread on agar; antibiotic disks are placed on the surface; zones of inhibition are measured to determine susceptibility.

Results are compared to reference tables and summarized in an antibiogram.
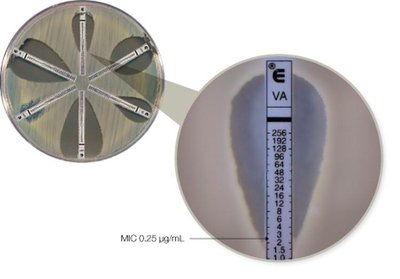
E-test
Uses strips with a gradient of antibiotic concentration; determines minimum inhibitory concentration (MIC).
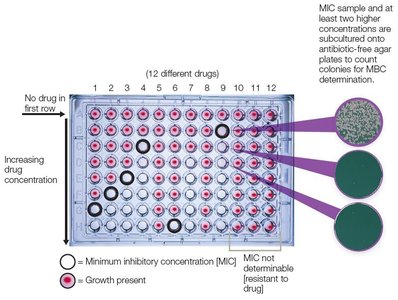
Broth Dilution Test
Serial dilutions of antibiotics in broth; MIC is the lowest concentration preventing visible growth; MBC is determined by subculturing to antibiotic-free media.
Antimicrobial Resistance and Stewardship
Types of Resistance
Intrinsic resistance: Natural property of certain microbes (e.g., lack of cell wall, impermeable outer membrane, biofilm formation).
Acquired resistance: Due to genetic mutation or acquisition of resistance genes (via horizontal gene transfer).
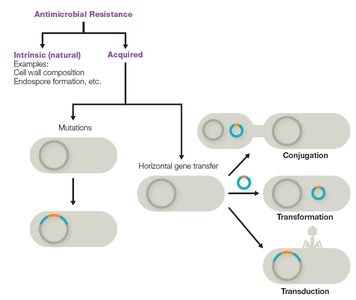
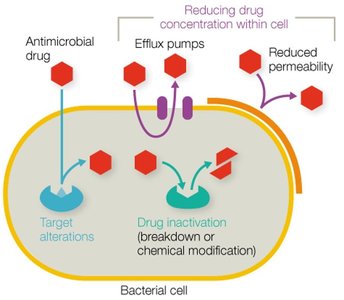
Mechanisms of Acquired Resistance
1. Altering the drug’s target (e.g., mutation in RNA polymerase for rifampin resistance).
2. Inactivating the drug (e.g., beta-lactamases, acetyltransferases).
3. Reducing drug concentration inside the cell (e.g., efflux pumps, reduced permeability).
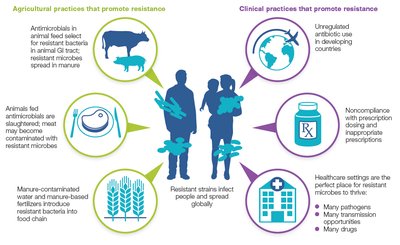
Development and Spread of Resistance
Resistance is accelerated by misuse and overuse of antimicrobials in clinical and agricultural settings.
Noncompliance with dosing, inappropriate prescriptions, and use in animal feed contribute to the problem.
Antimicrobial Stewardship
Healthcare workers should limit unnecessary prescriptions, use narrow-spectrum drugs when possible, and educate patients on proper use.
Patients should complete prescribed regimens and avoid self-medication.
Challenges in Drug Development
Developing new antimicrobials is costly, time-consuming, and less profitable than drugs for chronic conditions.
Strategies include combination therapies, resistance inhibitors, and phage therapy.
Visual Summary

