 Back
BackBacterial Pathogenesis and Selected Human Pathogens
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Bacterial Pathogenesis
Host-Parasite Relationships
Understanding the interaction between microbes and their hosts is fundamental to microbiology and infectious disease. The relationship can range from harmless colonization to severe disease.
Infection: The growth and multiplication of a parasite within or on a host. Infection may or may not result in overt disease.
Pathogen: Any parasitic organism that causes infectious disease. Primary (frank) pathogens cause disease by direct interaction with a healthy host, while opportunistic pathogens are often part of the normal flora and cause disease when they access other tissues or the host is immunocompromised.
Pathogenicity: The ability of a parasite to cause disease.
Robert Koch and Koch’s Postulates
Robert Koch was a pioneering German physician who established the foundational principles of microbial pathogenesis, known as Koch’s postulates. These criteria are used to link specific microorganisms to specific diseases.
1. The microorganism must be found in abundance in diseased individuals.
2. The microorganism must be isolated from the diseased individual and grown in pure culture.
3. The cultured microorganism must cause disease when introduced into a healthy organism (animal model).
4. The microorganism must be re-isolated from the experimentally infected host.
The Infectious Disease Process
Infectious diseases can be caused by viruses, bacteria, fungi, or protozoa. The process involves several stages and is characterized by specific signs and symptoms.
Signs: Objective changes in the body that can be directly observed (e.g., rash, fever).
Symptoms: Subjective changes experienced by the patient (e.g., pain, fatigue).
Disease Syndrome: A set of characteristic signs and symptoms associated with a disease.
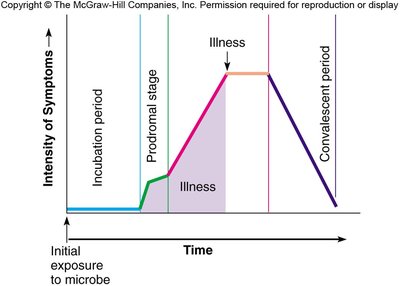
Course of Infectious Disease
The progression of an infectious disease typically follows a predictable pattern:
Incubation Period: Time between pathogen entry and appearance of signs and symptoms.
Prodromal Stage: Onset of nonspecific signs and symptoms, not yet diagnostic.
Period of Illness: Disease is most severe with characteristic signs and symptoms.
Convalescence: Signs and symptoms begin to disappear as recovery occurs.
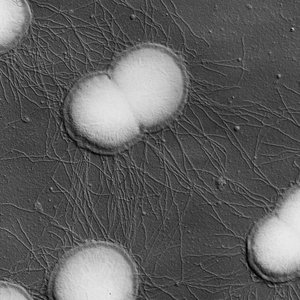
Neisseria gonorrhoeae
General Characteristics
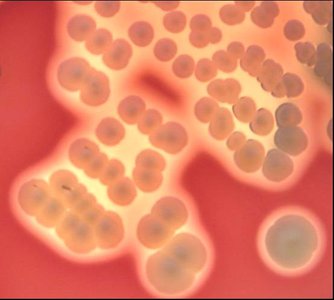
Neisseria gonorrhoeae is a Gram-negative diplococcus, commonly referred to as gonococcus. It is the causative agent of the sexually transmitted infection gonorrhea.
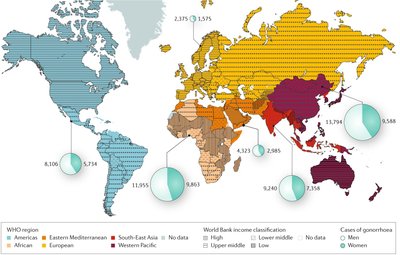
Colonizes the urethra in men and the cervix in women (less commonly the fallopian tubes, uterus, or urethra in women).
Highest incidence in the African WHO region; lowest in the European region.
Antibiotic Resistance
Some strains of N. gonorrhoeae have developed resistance to multiple antibiotics, including azithromycin and ceftriaxone, leading to the emergence of so-called "super-gonorrhea." Treatment options are becoming limited, though some strains remain sensitive to ertapenem.
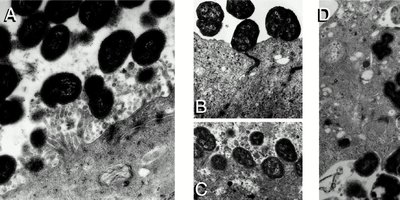
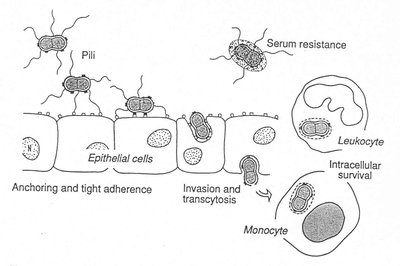
Pathogenesis
The pathogenesis of N. gonorrhoeae involves several steps, including adherence to epithelial cells, invasion, and evasion of the immune system.
Early infection involves microcolony formation on epithelial surfaces, followed by dispersal and monolayer adherence.
Bacteria increase contact with host cell membranes, traverse the epithelium, and induce inflammation.
Surface proteins inactivate complement, and the bacteria can survive phagocytosis by macrophages, exiting as immune-resistant forms.
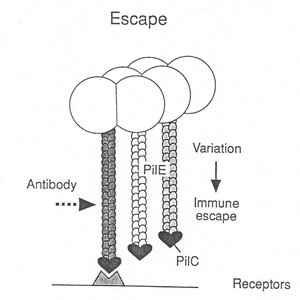
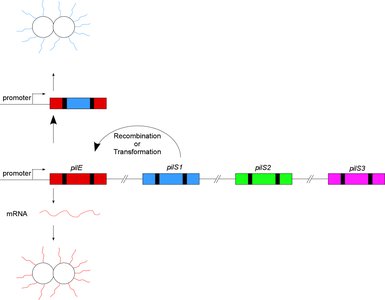
Immune Evasion: Pilin Phase Variation
N. gonorrhoeae can escape the adaptive immune response by varying the amino acid sequence of its pilin proteins, a process known as phase variation. This allows the bacteria to avoid antibody recognition.
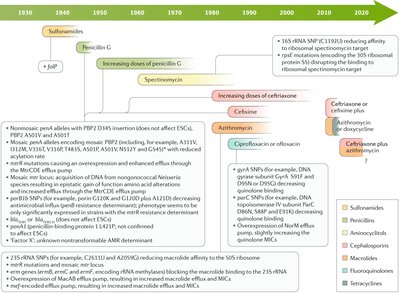
Treatment and Resistance Timeline
The treatment of gonorrhea has evolved due to the development of antibiotic resistance. The timeline below summarizes the introduction and resistance to various antibiotics.
Antibiotic | Year Introduced | Resistance Emergence |
|---|---|---|
Sulfonamides | 1930s | 1940s |
Penicillin G | 1940s | 1950s |
Spectinomycin | 1960s | 1970s |
Ceftriaxone | 1980s | 2010s |
Azithromycin | 1990s | 2010s |
Staphylococcus aureus
General Characteristics
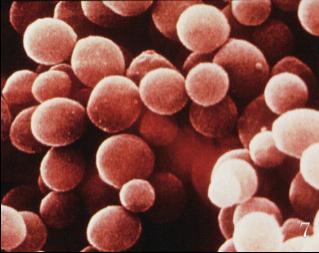
Staphylococcus aureus is a Gram-positive coccus, often appearing in clusters resembling grapes. It is a major nosocomial (hospital-acquired) pathogen and can cause a variety of diseases.
Commensal organism; 20% of people are stably colonized, 60% are intermittent carriers.
Causes skin and soft tissue infections, toxin-mediated diseases, surgical site infections, osteomyelitis, pneumonia, endocarditis, and keratitis.


Pathogenesis and Virulence Factors
S. aureus employs multiple strategies to acquire nutrients, evade the immune system, and damage host tissues.
Extracts iron from hosts using siderophores and heme extraction systems.
Produces a variety of toxins (e.g., α-toxin, β-toxin, δ-toxin, TSST-1) and enzymes (proteases, nucleases, lipases).
Forms biofilms, which protect against immune responses and antibiotics.
Regulates virulence gene expression via the accessory gene regulator (agr) quorum sensing system.
Clinical Manifestations
Abscesses: Localized collections of pus due to infection.
Folliculitis: Infection of hair follicles.
Osteomyelitis: Infection of bone.
Stye: Infection of eyelid glands.
Scalded Skin Syndrome: Toxin-mediated blistering skin disease.


Antibiotic Resistance
S. aureus has developed resistance to multiple antibiotics, including penicillin and methicillin (MRSA). Methicillin resistance is mediated by the mecA gene, which encodes a penicillin-binding protein (PBP2a) with low affinity for β-lactam antibiotics.
Regulation involves the BlaR1 sensor and BlaI repressor.
Vancomycin-resistant strains (VRSA) have also emerged.
Vibrio cholerae and Cholera
General Characteristics and Historical Impact
Vibrio cholerae is a Gram-negative bacterium responsible for cholera, a severe diarrheal disease. Cholera has had significant historical and evolutionary impacts, including a possible link to the prevalence of cystic fibrosis mutations.
Pathogenesis
Cholera pathogenesis is mediated by the cholera toxin, which is encoded by a bacteriophage. The toxin consists of two subunits (A and B) and acts by increasing cAMP levels in intestinal cells, leading to massive water and electrolyte loss ("rice-water stool").
Toxin-coregulated pilus (TCP) allows for microcolony formation and serves as a receptor for the CTX phage.
Symptoms include severe diarrhea, dehydration, and electrolyte imbalance.
Treatment and Prevention
Oral or intravenous rehydration salts are the mainstay of treatment.
Vaccines (e.g., RTS,S) are available and can provide partial protection.
Mycobacterium tuberculosis and Tuberculosis
General Characteristics
Mycobacterium tuberculosis is an acid-fast, Gram-positive, obligate aerobe discovered by Robert Koch. Its cell wall contains mycolic acids, which confer resistance to desiccation and many antibiotics.
Pathogenesis and Host Response
Infection leads to granuloma formation, a host strategy to contain the bacteria.
Treatment for latent infection includes isoniazid; active infection is treated with a combination of isoniazid, rifampin, ethambutol, and pyrazinamide.
Yersinia pestis and Plague
General Characteristics and Transmission
Yersinia pestis is the causative agent of plague, transmitted primarily by fleas. It infects lymphoid tissue and can cause bubonic, septicemic, or pneumonic plague.
Pathogenesis
Virulence is mediated by a plasmid encoding a type III secretion system, which injects Yersinia outer proteins (Yops) into host cells to disrupt phagocytosis and immune responses.
Treatment includes gentamicin and fluoroquinolones; attenuated strains are used in research.
Eukaryotic Pathogens
Malaria (Plasmodium spp.)
Malaria is caused by Plasmodium species and transmitted by female Anopheles mosquitoes. The parasite undergoes a complex life cycle involving liver and red blood cell stages.
Symptoms include periodic fever, chills, anemia, and organ enlargement.
Diagnosis is by microscopy or serology; treatment includes antimalarial drugs (quinine, chloroquine, atovaquone/proguanil).
Prevention includes bed nets, insecticides, and vaccination (RTS,S vaccine).
Sickle-Cell Disease and Malaria Resistance
Sickle-cell disease is caused by a mutation in the hemoglobin gene, resulting in abnormal red blood cells. Individuals with sickle-cell trait are resistant (but not immune) to malaria because infected cells lyse before the parasite can replicate extensively.
Leishmaniasis
Leishmaniasis is caused by Leishmania species and transmitted by sand flies. It exists in cutaneous and visceral forms, with the latter being potentially fatal without treatment.
Diagnosis is by observation of parasites in macrophages; treatment includes miltefosine and other antiparasitic drugs.
Chagas Disease (Trypanosoma cruzi)
Chagas disease is caused by Trypanosoma cruzi and transmitted by triatomine bugs. It has acute and chronic phases, with the latter causing heart and gastrointestinal complications.
Treatment is effective in the acute phase (benznidazole, nifurtimox) but not in the chronic phase.
African Sleeping Sickness (Trypanosoma brucei)
African sleeping sickness is caused by Trypanosoma brucei and transmitted by tsetse flies. It progresses from blood infection to central nervous system involvement, leading to behavioral changes and coma.
Treatment includes suramin, melarsoprol, and pentamidine.
