 Back
BackCh 10 - Controlling Microbial Growth in the Body: Antimicrobial Drugs
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Controlling Microbial Growth in the Body: Antimicrobial Drugs
The History of Antimicrobial Agents
The development of antimicrobial drugs revolutionized the treatment of infectious diseases. Key historical figures contributed to the discovery and advancement of these agents.
Paul Ehrlich: Proposed the concept of "magic bullets"—chemicals that selectively target pathogens. Discovered arsenic compounds effective against microbes.
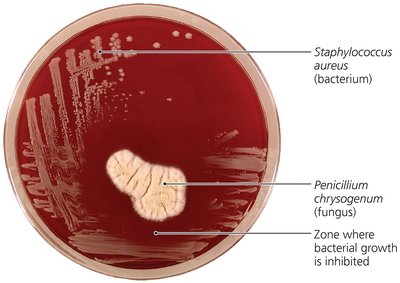
Alexander Fleming: Discovered penicillin, the first true antibiotic, produced by the mold Penicillium chrysogenum.
Gerhard Domagk: Discovered sulfanilamide, the first widely used synthetic antimicrobial.
Selman Waksman: Coined the term "antibiotics" for antimicrobial agents produced naturally by organisms.
Definitions:
Antibiotics: Antimicrobial agents produced naturally by microorganisms.
Synthetics: Antimicrobials completely synthesized in the laboratory.
Semisynthetics: Chemically modified antibiotics that are more effective, longer lasting, or easier to administer.
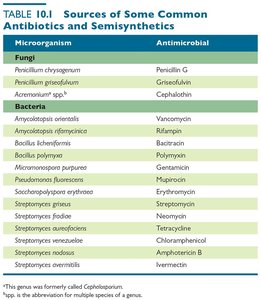
Sources of Common Antibiotics and Semisynthetics
Many antibiotics are derived from fungi and bacteria. The following table summarizes some important sources:
Microorganism | Antimicrobial |
|---|---|
Penicillium chrysogenum | Penicillin G |
Penicillium griseofulvum | Griseofulvin |
Acremonium spp. | Cephalothin |
Amycolatopsis orientalis | Vancomycin |
Bacillus polymyxa | Polymyxin |
Streptomyces griseus | Streptomycin |
Streptomyces aureofaciens | Tetracycline |
Streptomyces avermitilis | Ivermectin |
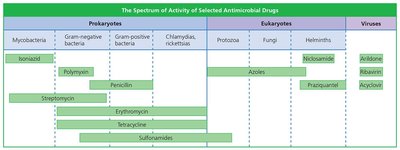
Principle of Selective Toxicity
Selective toxicity is the ability of an antimicrobial drug to harm the pathogen without harming the host. This principle is fundamental to the effectiveness and safety of antimicrobial therapy.
Antibacterial drugs are the most numerous and diverse due to the significant differences between bacterial and human cells.
Fewer drugs are available for eukaryotic pathogens (fungi, protozoa, helminths) and viruses due to similarities with human cells.
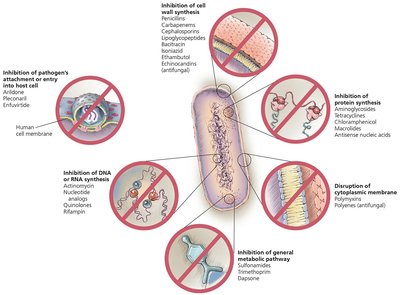
Mechanisms of Antimicrobial Action
Antimicrobial drugs target specific structures or functions in microbes. The six main mechanisms are:
Inhibition of cell wall synthesis
Inhibition of protein synthesis
Disruption of cytoplasmic membrane
Inhibition of general metabolic pathways
Inhibition of DNA or RNA synthesis
Inhibition of pathogen's attachment or entry into host cell
Inhibition of Cell Wall Synthesis
Many antibiotics target the synthesis of peptidoglycan, a key component of bacterial cell walls. This weakens the wall, causing cell lysis.
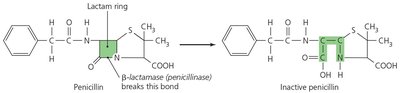
Beta-lactams (e.g., penicillins, cephalosporins, carbapenems) bind to enzymes that cross-link NAM subunits, preventing proper cell wall formation.
Vancomycin and cycloserine interfere with bridges between NAM subunits in Gram-positive bacteria.
Bacitracin blocks transport of NAG and NAM from the cytoplasm.
Isoniazid and ethambutol disrupt mycolic acid formation in mycobacteria.

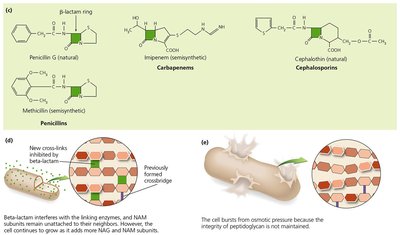
Note: These drugs are effective only against growing cells and do not affect existing peptidoglycan.
Inhibition of Fungal Cell Wall Synthesis
Fungal cell walls contain unique polysaccharides. Echinocandins inhibit glucan synthesis, weakening the fungal cell wall.
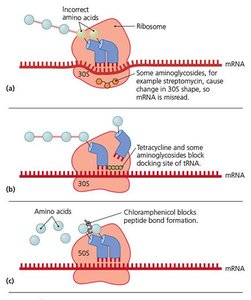
Inhibition of Protein Synthesis
Antimicrobials can selectively target prokaryotic ribosomes (70S) without affecting eukaryotic ribosomes (80S), though mitochondrial ribosomes may be affected.

Aminoglycosides (e.g., streptomycin) cause misreading of mRNA.
Tetracyclines block tRNA docking.
Chloramphenicol blocks peptide bond formation.
Macrolides and lincosamides block ribosomal movement.
Oxazolidinones block initiation of translation.

Mupirocin selectively binds isoleucyl-tRNA synthetase, preventing isoleucine incorporation in Gram-positive bacteria.
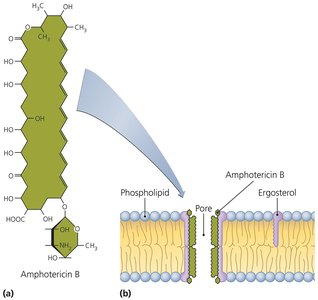
Disruption of Cytoplasmic Membranes
Some drugs disrupt membrane integrity, causing cell death.
Polymyxins disrupt Gram-negative bacterial membranes (toxic to human kidneys).
Nystatin and amphotericin B bind to ergosterol in fungal membranes, forming pores.
Azoles and allylamines inhibit ergosterol synthesis in fungi.
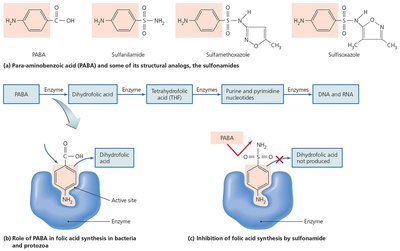
Inhibition of Metabolic Pathways
Antimetabolic agents target pathways unique to pathogens.
Sulfonamides are structural analogs of PABA, blocking folic acid synthesis in bacteria and protozoa.
Trimethoprim interferes with nucleotide synthesis.
Atovaquone disrupts electron transport in protozoa and fungi.
Antiviral agents (amantadine, rimantadine) prevent viral uncoating; protease inhibitors block HIV replication.
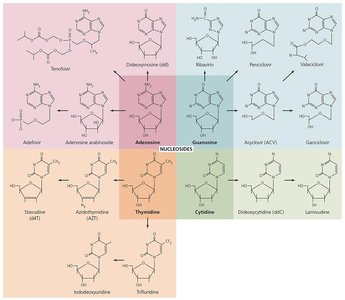
Inhibition of Nucleic Acid Synthesis
Some drugs block DNA replication or RNA transcription, often affecting both prokaryotic and eukaryotic cells.
Quinolones and fluoroquinolones inhibit DNA gyrase in bacteria.
Nucleotide/nucleoside analogs distort nucleic acid shapes, preventing replication and transcription (used against viruses and cancer cells).
Reverse transcriptase inhibitors target HIV-specific enzymes.
Prevention of Virus Attachment, Entry, or Uncoating
Attachment antagonists block viral proteins or host receptors, preventing infection. Examples include pleconaril (blocks attachment) and arildone (prevents uncoating).
Clinical Considerations in Prescribing Antimicrobial Drugs
Spectrum of Action
Antimicrobials vary in the range of pathogens they affect.
Narrow-spectrum drugs target a limited group of microbes.
Broad-spectrum drugs target a wide variety but may disrupt normal flora, leading to superinfections.
Effectiveness
Several laboratory tests assess antimicrobial efficacy:
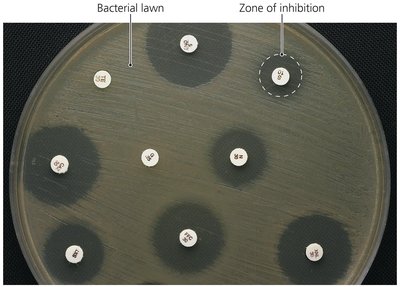
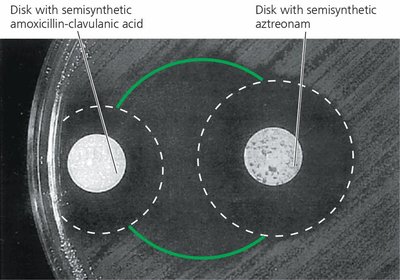
Diffusion susceptibility (Kirby-Bauer) test: Measures zones of inhibition around antibiotic disks.
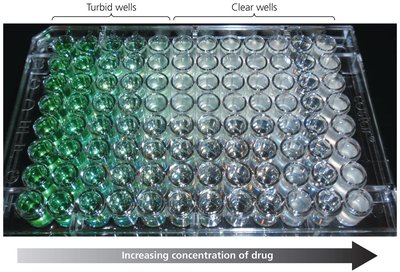
Minimum inhibitory concentration (MIC) test: Determines the lowest drug concentration that inhibits visible growth.
Minimum bactericidal concentration (MBC) test: Identifies the lowest concentration that kills the microbe.
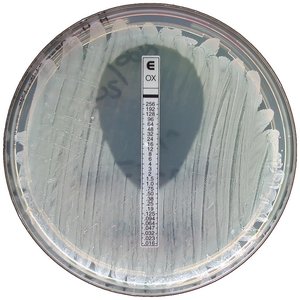
Etest: Combines aspects of Kirby-Bauer and MIC tests using a gradient strip.
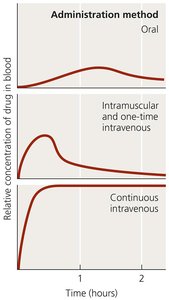
Routes of Administration
Antimicrobials can be administered in several ways, affecting their distribution and effectiveness:
Topical: For external infections.
Oral: Convenient, but absorption may be variable.
Intramuscular (IM): Delivers drug into muscle tissue.
Intravenous (IV): Directly into the bloodstream for rapid, high concentrations.
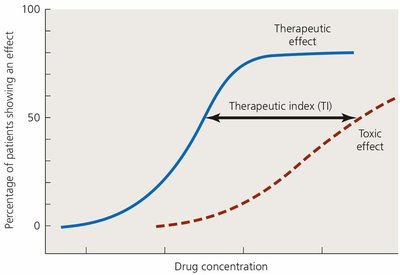
Safety and Side Effects
Toxicity: Some drugs are toxic to kidneys, liver, or nerves. The therapeutic index (TI) is the ratio of the tolerated dose to the effective dose. A higher TI indicates greater safety.
Allergies: Rare but can be severe (e.g., anaphylactic shock).
Disruption of normal microbiota: May lead to secondary infections or superinfections, especially in hospitalized patients.
Resistance to Antimicrobial Drugs
The Development of Resistance in Populations
Microbial resistance can arise through mutations or acquisition of resistance genes (often on R plasmids) via transformation, transduction, or conjugation.

Mechanisms of Resistance
Enzyme production that destroys or deactivates the drug (e.g., beta-lactamase).
Prevention of drug entry into the cell.
Alteration of drug target site.
Alteration of metabolic pathways.
Efflux pumps expel the drug from the cell.
Biofilm formation increases resistance.
Production of proteins that protect target enzymes (e.g., MfpA in Mycobacterium tuberculosis).
Multiple Resistance and Cross Resistance
Multiple resistance: Pathogens resistant to three or more antimicrobial agents, often due to R plasmid exchange.
Cross resistance: Resistance to drugs with similar structures or mechanisms.
Retarding Resistance
Maintain high drug concentrations in patients to inhibit pathogens.
Use combinations of antimicrobials (synergism enhances effect; antagonism reduces efficacy).
Limit antimicrobial use to necessary cases.
Develop new drugs and modify existing ones to overcome resistance.
Additional info: Continued research and responsible use of antimicrobials are essential to combat the growing threat of resistance.
