 Back
BackCurviform, Cell Wall-Deficient, and Obligate Intracellular Bacteria: Pathogenesis and Clinical Relevance
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Curviform Bacteria
Major Genera and General Features
Curviform bacteria are Gram-negative, enteric pathogens with distinctive curved or spiral shapes. The three major genera are Vibrio, Campylobacter, and Helicobacter. These organisms are important causes of gastrointestinal and systemic diseases in humans.
Vibrio: Comma-shaped, monotrichous flagella, facultative anaerobes, mostly halophilic (require extra salt), possess polar flagellum and pili, and have two chromosomes (unusual for bacteria).
Campylobacter: Curved rods or short spirals, monotrichous flagella, microaerophilic, and motile.
Helicobacter: Tight spirals, lophotrichous flagella, microaerophilic, and associated with gastric pathology.
Vibrio cholerae: Pathogenesis and Epidemiology
Vibrio cholerae is the causative agent of cholera, a severe diarrheal disease. It is characterized by over 200 O serotypes and produces several toxins, including cholera toxin (an A-B toxin) and accessory enterotoxins. The cholera toxin increases cAMP in intestinal cells, leading to massive fluid secretion and the characteristic "rice water stool." The infectious dose is high but decreases with reduced stomach acidity.
Transmission: Fecal-oral route, often via contaminated water or food.
Symptoms: Profuse watery diarrhea, dehydration, muscle and neurological symptoms.
Treatment: Oral rehydration therapy, tetracycline; a live attenuated vaccine is available but offers limited protection.
Epidemiology: Seven major pandemics; recent outbreaks have affected multiple countries with high morbidity and mortality.



Other Pathogenic Vibrios
Vibrio parahaemolyticus: Causes gastroenteritis from raw/undercooked shellfish; symptoms similar to cholera.
Vibrio vulnificus: Causes severe wound infections, especially in warm months; high mortality and risk of septicemia, particularly in immunocompromised individuals.
Diagnosis: Identification of curved Gram-negative rods in clinical specimens, selective media (TCBS agar), serotyping, and oxidase testing.
Campylobacter
General Features and Pathogenesis
Campylobacter species are small, curved, Gram-negative rods that are microaerophilic and motile. They are a leading cause of bacterial gastroenteritis in the United States, often transmitted through contaminated poultry and unpasteurized milk.
Virulence: Ability to burrow through mucus and multiply in the intestinal epithelium; some produce a heat-labile enterotoxin (CJT).
Clinical Manifestations: Gastroenteritis, with possible complications such as Guillain-Barré syndrome (autoimmune demyelination).
Treatment: Supportive care with rehydration; increasing antibiotic resistance is a concern.
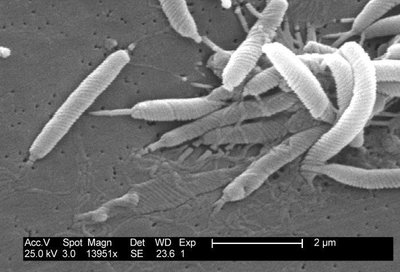
Helicobacter pylori
Pathogenesis and Clinical Importance
Helicobacter pylori is a microaerophilic, spiral-shaped bacterium with lophotrichous flagella. It is the primary cause of gastric and duodenal ulcers and is associated with an increased risk of stomach cancer. The bacterium produces urease, which neutralizes stomach acid, allowing colonization of the gastric mucosa.
Virulence Factors: Urease production, adhesion to gastric epithelium, and induction of inflammation.
Clinical Relevance: Responsible for 90% of peptic ulcers; people with type O blood are at slightly higher risk.
Historical Note: Discovery of H. pylori's role in ulcers was awarded the Nobel Prize in 2005.
Cell Wall-Deficient Bacteria: Mycoplasmatales
General Features
Members of the order Mycoplasmatales, including Mycoplasma and Ureaplasma, are the smallest free-living bacteria and lack cell walls. This makes them resistant to many antibiotics that target cell wall synthesis. They are pleomorphic, slow-growing, and difficult to identify in the laboratory.
Mycoplasma pneumoniae: Causes bronchitis and "walking pneumonia"; binds to ciliated respiratory cells and evades the immune system by changing surface proteins.
STI Mycoplasmas: M. genitalium, M. hominis, and U. urealyticum cause urogenital infections and are associated with reproductive complications. Rising drug resistance is a significant concern.
Obligate Intracellular Bacteria: Rickettsiaceae
General Features and Classification
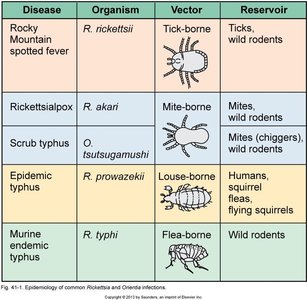
The family Rickettsiaceae includes small, Gram-negative, non-motile, pleomorphic bacteria that grow intracellularly, primarily in endothelial cells. They are transmitted by arthropod vectors and cause necrosis of infected tissues. There are two main groups: the spotted fever group and the typhus group.
Spotted Fever Group: Includes Rickettsia rickettsii (Rocky Mountain spotted fever) and Orientia species.
Typhus Group: Includes Rickettsia prowazekii (epidemic typhus), Rickettsia typhi (endemic typhus), and Orientia tsutsugamushi (scrub typhus).
Treatment: Doxycycline is the drug of choice for all rickettsioses.

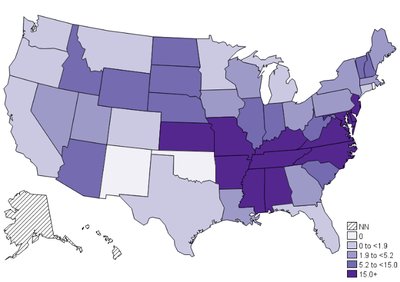
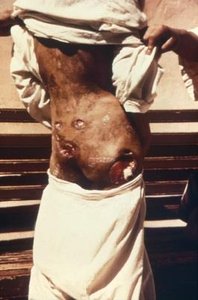
Rickettsia rickettsii: Rocky Mountain Spotted Fever (RMSF)
R. rickettsii is the most common severe or fatal tick-borne disease in the US. It adheres to host cells via OmpA, invades endothelial cells, and causes a characteristic rash and systemic symptoms. Early treatment is critical to prevent severe complications and death.
Symptoms: Fever, headache, vomiting, muscle aches, and a rash that appears 2-5 days after onset.
Diagnosis: Giemsa stain, PCR from rash sites, and microimmunofluorescence (MIF).
Prevention: Use of insect repellent, protective clothing, and prompt tick removal.



Other Rickettsial Diseases
Rickettsia parkeri: Transmitted by Gulf Coast ticks; causes a milder RMSF-like illness with eschar at the bite site.
Rickettsia akari: Causes rickettsialpox, transmitted by mites; biphasic illness with vesicular rash.
Rickettsia prowazekii: Causes epidemic typhus, transmitted by body lice; associated with crowded, unsanitary conditions and high mortality if untreated.
Rickettsia typhi: Causes endemic (murine) typhus, transmitted by fleas; milder disease, common in warm, humid areas.
Orientia tsutsugamushi: Causes scrub typhus, transmitted by chiggers; can be severe, especially in older or immunocompromised individuals.


Obligate Intracellular Bacteria: Chlamydiaceae
General Features and Life Cycle
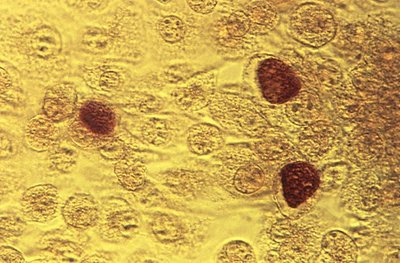
Chlamydiaceae are very small, obligate intracellular bacteria with a Gram-negative-like cell wall but low peptidoglycan. They have a unique biphasic life cycle, alternating between infectious elementary bodies (EBs) and replicative reticulate bodies (RBs).
Elementary Body (EB): Infectious, metabolically inactive form that survives outside host cells.
Reticulate Body (RB): Intracellular, metabolically active, and replicative form.

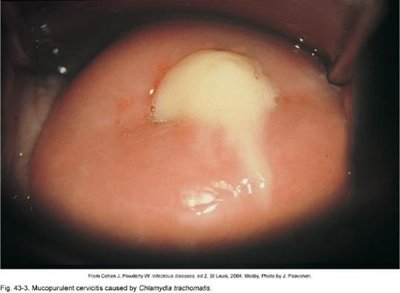
Chlamydia trachomatis: Clinical Manifestations
Chlamydia trachomatis is the most common bacterial sexually transmitted infection (STI) worldwide. It infects mucous membranes, causing urethritis, cervicitis, pelvic inflammatory disease (PID), and can lead to infertility. It also causes inclusion conjunctivitis and infant pneumonia.
Ocular trachoma: Chronic infection leading to eyelid and corneal deformation, and potentially blindness.
Lymphogranuloma venereum (LGV): Severe, disfiguring infection of genitalia and lymphatics.



Diagnosis and Treatment of Chlamydia
Diagnosis: NAATs (nucleic acid amplification tests), immunofluorescence, and Giemsa stain for inclusion bodies. Culture is rarely performed due to cost and complexity.
Treatment: Doxycycline is preferred; beta-lactam antibiotics are ineffective. Barrier protection (condoms, dental dams) is essential for prevention.

Other Chlamydiaceae
Chlamydophila psittaci: Causes psittacosis (ornithosis), a zoonotic infection from birds; treated with macrolides.
Chlamydophila pneumoniae: Causes respiratory infections; diagnosis is challenging and often relies on immunofluorescence.
Waddlia chondrophila: Emerging pathogen associated with miscarriages and possibly respiratory infections; no commercial tests available.
