 Back
BackCytopathology of the Female Genital Tract: Microbiological and Cellular Perspectives
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Cytology and Cervical Screening
Introduction to Cytology
Cytology is the study of cells, focusing on their structure, function, and pathology. In the context of the female genital tract, cytology is primarily used for cervical screening to detect pre-cancerous and cancerous changes in cervical cells. The main aim of cervical screening is to reduce the incidence and mortality of cervical cancer by identifying and monitoring cellular abnormalities before they progress to malignancy.
Non-Gynae Cytology: Analysis of urine, body fluids, and fine needle aspirates (FNA).
Gynae Cytology: Involves scraping or brushing cells from the cervix for examination.
Cervical Screening Programme
The NHS Cervical Screening Programme is a public health initiative designed to systematically screen women and people with a cervix, aiming for early detection of cervical abnormalities. The programme has evolved over time, incorporating technological advances and expanding eligibility.
Introduced in 1964, with major updates in 1988 (computerised recall), 2004 (liquid-based cytology), 2008 (HPV vaccination), and 2019 (primary HPV testing).
Eligibility: People aged 25–64 with a cervix, with opt-in options for trans men.
Coverage target: 80% (recent rates ~68–70%).
Cervical Epithelium and Menstrual Cycle
Structure of Cervical Epithelium
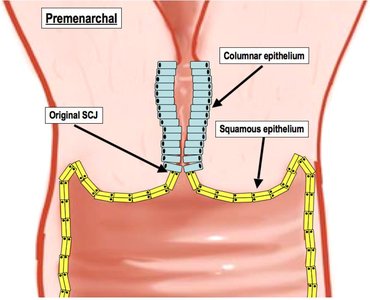
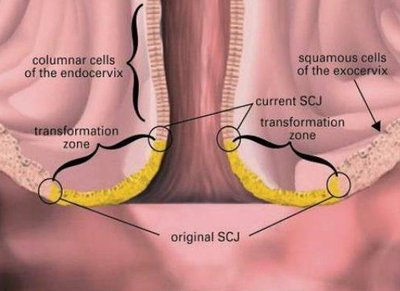
The cervix is lined by two main types of epithelium: the ectocervix (stratified squamous epithelium) and the endocervix (single-layered columnar epithelium). The interface between these is the squamo-columnar junction (SCJ), which is clinically significant as the most common site for cervical neoplasia.
Ectocervix: Multilayered squamous epithelium.
Endocervix: Single layer of columnar epithelium.
SCJ: Dynamic location, moves with age and hormonal changes.
Hormonal Influence and Sampling Timing
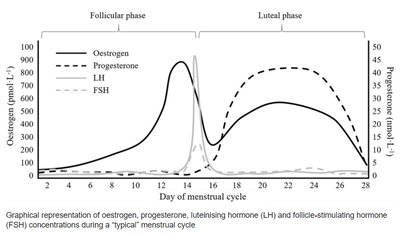
The cervical epithelium responds to hormonal changes, particularly oestrogen and progesterone, during the menstrual cycle. The optimal time for sampling is days 10–14, when oestrogen peaks and the epithelium is at full thickness.
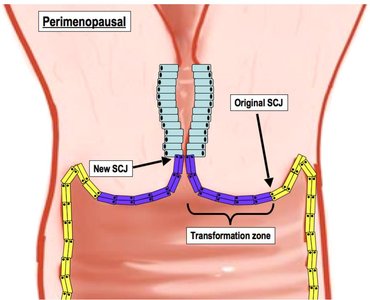
Squamo-Columnar Junction (SCJ) and Transformation Zone (TZ)
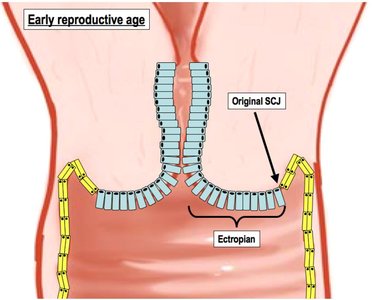
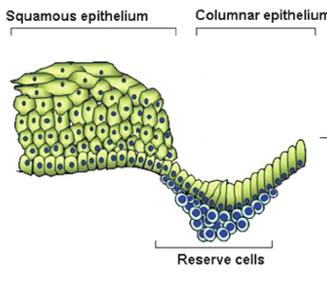
The SCJ shifts position throughout life, especially during puberty, reproductive years, and menopause. The transformation zone (TZ) is the area between the old and new SCJ, where columnar cells are replaced by metaplastic squamous cells due to the acidic vaginal environment. This zone is the most susceptible to neoplastic transformation.
Sample Collection and Processing
Sample Collection Techniques
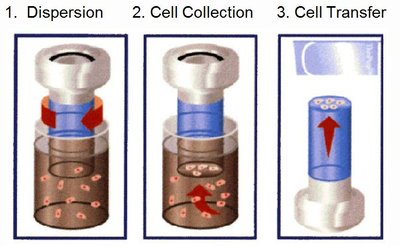
Accurate sampling of the transformation zone is critical for effective screening. Conventional cytology uses Ayres/Aylesbury spatulas, while liquid-based cytology (LBC) uses a Cervex brush and fixative vial. LBC offers improved cell preservation and lower inadequate rates.
Conventional cytology: Direct smear on slide, spray-fixed.
LBC: Cells suspended in fixative, processed for higher quality slides.


Automated Cytology Processing
Modern cytology laboratories use automated machines for slide preparation and staining, such as the Hologic T5000 and Prisma. The Papanicolaou stain is standard, highlighting nuclear and cytoplasmic features for microscopic evaluation.

HPV and Molecular Testing
HPV Vaccination and Screening
Human papillomavirus (HPV) is implicated in over 80% of cervical cancers, especially types 16 and 18. Vaccination programmes (Gardasil and Gardasil 9) target multiple high-risk HPV types and are offered to both girls and boys. Screening remains necessary even after vaccination due to incomplete coverage of all oncogenic HPV types.
HPV Molecular Testing
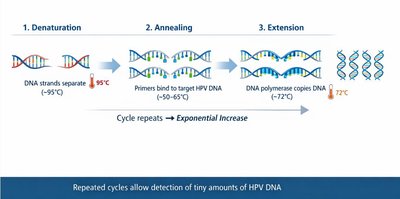
HPV testing uses polymerase chain reaction (PCR) to detect high-risk HPV DNA in cervical samples. Since 2019, primary HPV testing is standard in the UK screening programme, with cytology used as a reflex test if HPV is detected.
Detects 14 high-risk HPV subtypes.
PCR process: Denaturation, annealing, extension.

Normal and Abnormal Cytology
Normal Epithelial Cell Types
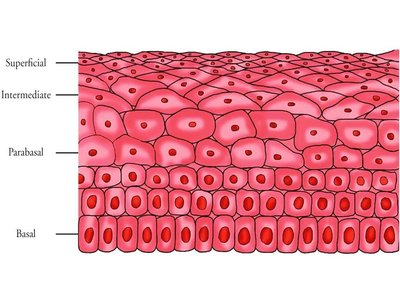
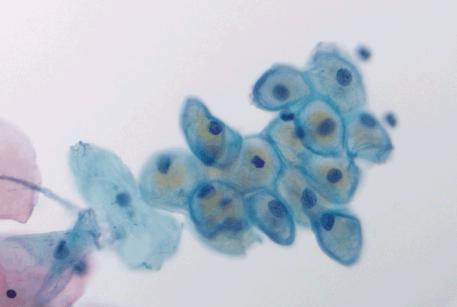
Understanding normal cell morphology is essential for identifying abnormalities. The main epithelial cell types found in cervical cytology are:
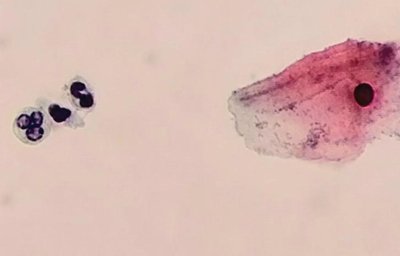
Superficial cells: Polygonal, pink/orange, small pyknotic nucleus.
Intermediate cells: Oval, blue cytoplasm, larger nucleus.
Parabasal cells: Small, round, dense blue cytoplasm, high nuclear:cytoplasmic ratio.
Metaplastic cells: Round/oval, dense blue, large nucleus, nucleoli present.
Endocervical cells: Oval/round nucleus, foamy blue/green cytoplasm, cilia may be present.
Endometrial cells: Eccentric nuclei, scant cytoplasm, variable size/shape, often in clusters.

Infectious Agents in Cervical Cytology
Common infections detected in cervical cytology include:
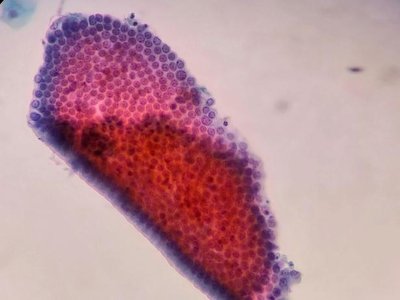
Candida albicans: Fungal hyphae and spores, red-staining walls.
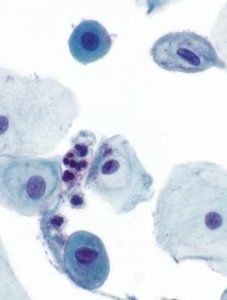
Actinomyces-like organisms: Dense basophilic balls, associated with intrauterine devices (IUDs).
Trichomonas vaginalis: Pear-shaped protozoa, blue cytoplasm, ill-defined nucleus.
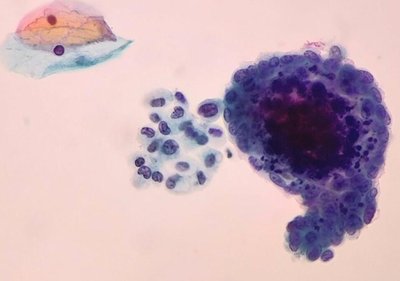
Herpes simplex virus: Intranuclear inclusions, ground glass nuclei, nuclear enlargement.
Inflammation and Cellular Changes
Inflammatory changes can affect all cell types, leading to nuclear enlargement, multinucleation, smooth nuclear membranes, and perinuclear halos. These changes must be distinguished from dyskaryosis.
Squamous and Glandular Abnormalities
Abnormalities are graded based on nuclear and cytoplasmic changes:
Squamous dyskaryosis: Increased nuclear:cytoplasmic ratio, irregular nuclear outlines, hyperchromasia, abnormal chromatin.
Low grade: n:c up to 50%, mild irregularities.
Moderate grade: n:c up to 75%, more pronounced changes.
Severe grade: n:c >75%, highly irregular nuclei, possible invasion.
Glandular abnormalities: Nuclear enlargement, hyperchromasia, coarse chromatin, mitoses, architectural changes.
Colposcopy and Future Directions
Role of Colposcopy
Patients with abnormal cytology are referred for colposcopy, where biopsies are taken for histological diagnosis and management. Results are classified as Cervical Intraepithelial Neoplasia (CIN) grades 1–3 or glandular neoplasia. Multidisciplinary team meetings ensure accurate diagnosis and patient care.
Future Developments
Emerging trends include self-sampling, digital cytology, and expanded molecular testing, aiming to improve screening accuracy and accessibility.
