 Back
BackDisorders Associated with the Immune System: Hypersensitivity, Autoimmunity, Transplantation, and AIDS
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Disorders Associated with the Immune System
Overview
This chapter explores the mechanisms and clinical implications of immune system disorders, including hypersensitivity reactions, autoimmune diseases, transplantation immunology, immunodeficiencies, and HIV/AIDS. Understanding these processes is essential for recognizing how the immune system can malfunction, leading to disease.
Hypersensitivity
Definition and Types
Hypersensitivity refers to an antigenic response beyond what is considered normal, occurring when an individual previously sensitized to an antigen (allergen) is re-exposed. There are four major types of hypersensitivity reactions, each with distinct mechanisms and clinical manifestations.
Type I (Anaphylactic): Immediate, IgE-mediated reactions.
Type II (Cytotoxic): Antibody-mediated cell destruction.
Type III (Immune Complex): Immune complex deposition and inflammation.
Type IV (Delayed Cell-Mediated): T cell-mediated delayed reactions.
Hygiene hypothesis: Suggests that reduced exposure to pathogens may lower immune tolerance and increase hypersensitivity to harmless antigens.
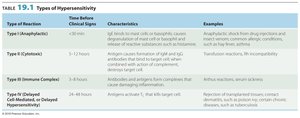
Type I (Anaphylactic) Reactions
These reactions occur within minutes of re-exposure to an allergen. IgE antibodies bind to mast cells and basophils, causing degranulation and release of mediators such as histamine, leukotrienes, and prostaglandins.
Histamine: Increases capillary permeability, leading to swelling and redness.
Leukotrienes: Prolonged contraction of smooth muscles (e.g., bronchospasm).
Prostaglandins: Affect smooth muscle and increase mucus secretion.

Systemic vs. Localized Anaphylaxis
Systemic anaphylaxis (anaphylactic shock): Severe, life-threatening reaction; may cause circulatory collapse and death. Treated with epinephrine.
Localized anaphylaxis: Usually due to inhaled or ingested allergens; symptoms depend on the route (e.g., hives, hay fever, asthma).

Diagnosis and Prevention of Anaphylactic Reactions
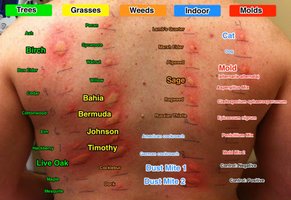
Skin tests: Allergens are injected or scratched into the skin to observe for a rapid inflammatory reaction (wheal).
Desensitization: Repeated, increasing doses of allergen are administered to induce IgG (blocking antibodies) that neutralize the allergen before it binds IgE.


Type II (Cytotoxic) Reactions
These reactions involve IgG or IgM antibodies binding to antigens on cell surfaces, activating complement and leading to cell lysis or damage by phagocytes.
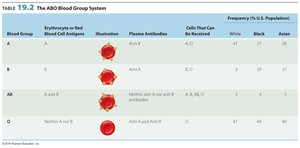
ABO blood group system: Antibodies form against A or B antigens on red blood cells (RBCs). Type O has no antigens and is the universal donor; type AB is the universal acceptor.
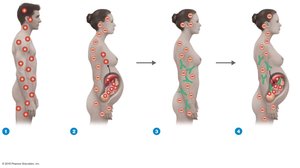
Rh Blood Group System and Hemolytic Disease of the Newborn (HDNB)
Rh factor: Present in 85% of the population (Rh+). Rh– individuals can develop anti-Rh antibodies after exposure to Rh+ blood.
HDNB: Occurs when an Rh– mother carries an Rh+ fetus; maternal anti-Rh antibodies attack fetal RBCs in subsequent pregnancies.
Drug-Induced Cytotoxic Reactions
Thrombocytopenic purpura: Platelets bind drugs, forming antigenic complexes that are destroyed by antibodies and complement.
Agranulocytosis: Immune destruction of granulocytes.
Hemolytic anemia: Immune destruction of RBCs.
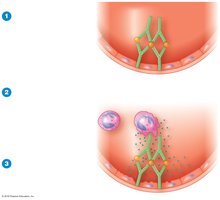
Type III (Immune Complex) Reactions
Antibodies form complexes with soluble antigens, which deposit in tissues and activate complement, causing inflammation and tissue damage.
Glomerulonephritis: Immune complexes deposit in kidney glomeruli, causing inflammation.
Type IV (Delayed Cell-Mediated) Reactions
These reactions are mediated by T cells and occur 24–48 hours after exposure. Antigens are processed by antigen-presenting cells and presented to T cells, which release cytokines upon re-exposure, causing tissue damage.
Allergic contact dermatitis: Haptens (e.g., urushiol from poison ivy) bind skin proteins, triggering T cell-mediated inflammation.


Autoimmune Diseases
Mechanisms and Types
Autoimmunity is the loss of self-tolerance, where the immune system attacks self-antigens, causing organ or tissue damage. Mechanisms include cytotoxic, immune complex, and cell-mediated reactions.
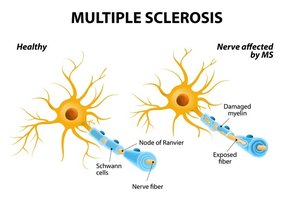
Cytotoxic: Antibodies react with cell-surface antigens (e.g., multiple sclerosis, Graves' disease, myasthenia gravis).
Immune complex: Immune complexes deposit in tissues (e.g., systemic lupus erythematosus, rheumatoid arthritis).
Cell-mediated: T cells attack self-tissues (e.g., type 1 diabetes, psoriasis).
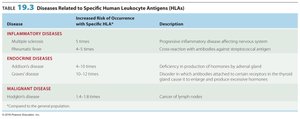
Reactions Related to the Human Leukocyte Antigen (HLA) Complex
HLA Complex and Disease Susceptibility
The human leukocyte antigen (HLA) complex encodes self-antigens on cell surfaces. Certain HLA types are associated with increased risk for specific diseases. HLA typing is essential for tissue matching in transplantation.
Transplantation Immunology
Transplant rejection: Mediated by T cells, macrophages, and antibodies against non-self HLAs.
Privileged sites/tissues: Locations (e.g., cornea, heart valves) less likely to elicit immune responses.

Stem Cells in Transplantation
Stem cells are undifferentiated cells capable of generating various cell types. Embryonic stem cells are pluripotent, while adult stem cells can be induced to pluripotency. Stem cells are used to regenerate tissues and organs.

Types of Grafts
Autograft: Tissue from the same individual.
Isograft: Tissue from an identical twin.
Allograft: Tissue from another person.
Xenotransplant: Tissue from another species (e.g., pig heart valve).


Graft-versus-Host Disease (GVHD)
GVHD occurs when transplanted bone marrow contains immunocompetent cells that attack the recipient's tissues.
The Immune System and Cancer
Immune Surveillance and Evasion
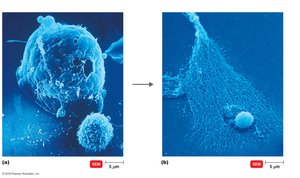
The immune system can recognize and destroy cancer cells via cytotoxic T lymphocytes (CTLs) and macrophages. However, tumors may evade detection by lacking antigenic epitopes, rapid growth, or becoming vascularized.
Immunotherapy
Bacterial endotoxins: Stimulate TNF to interfere with tumor blood supply.
Vaccines: Used for prophylaxis (e.g., HPV, hepatitis B).
Monoclonal antibodies: Target tumor antigens (e.g., Herceptin for breast cancer).
Immunotoxins: Monoclonal antibody linked to a toxin, selectively killing tumor cells.
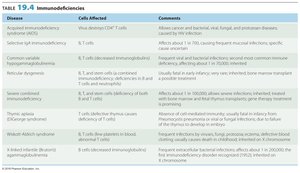
Immunodeficiencies
Types and Examples
Immunodeficiencies are conditions where the immune response is insufficient. They can be congenital (genetic) or acquired (due to infections, drugs, or cancers).
Congenital: Due to defective or missing genes (e.g., DiGeorge syndrome, SCID).
Acquired: Develop during life (e.g., AIDS, immunosuppressive therapy).
Acquired Immunodeficiency Syndrome (AIDS)
Origin and Structure of HIV
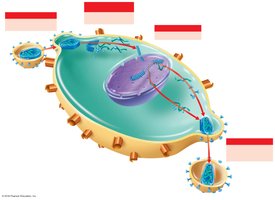
HIV is a retrovirus that infects CD4+ T cells, leading to immune deficiency. It originated from primates and was first identified in the early 1980s. The virus contains two RNA strands, reverse transcriptase, and glycoprotein spikes (gp120, gp41).

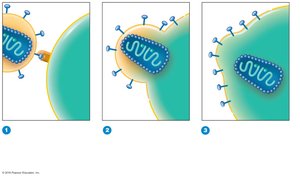
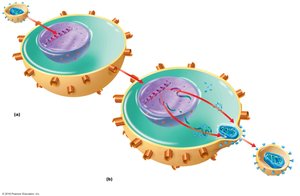
HIV Infection Mechanism
HIV binds to CD4 and CCR5/CXCR4 coreceptors on T cells, enters via fusion, and releases its RNA.
Reverse transcriptase synthesizes DNA from RNA, which integrates into the host genome as a provirus.
Active infection produces new viruses; latent infection hides the provirus in host DNA.

HIV Subtypes
HIV-1: Most common worldwide; related to chimpanzee viruses.
HIV-2: Less pathogenic, mainly in West Africa; related to sooty mangabey viruses.
Stages of HIV Infection
Phase 1: Asymptomatic or lymphadenopathy.
Phase 2: Gradual decline in CD4+ T cells; minor symptoms.
Phase 3 (AIDS): CD4+ T cell count < 200/μl; severe opportunistic infections and cancers.

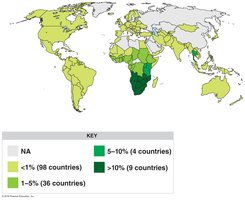
HIV Transmission and Epidemiology
Transmitted via sexual contact, blood, breast milk, transplacental infection, contaminated needles, and organ transplants.
Most cases are in sub-Saharan Africa; heterosexual transmission is predominant globally.
Prevention and Treatment of HIV/AIDS
Prevention: Safe sex, sterile needles, screening blood products.
Treatment: Antiretroviral therapy (ART) targets multiple stages of the HIV life cycle.
Drug classes include fusion/entry inhibitors, reverse transcriptase inhibitors (NRTIs, NNRTIs), integrase inhibitors, protease inhibitors, and maturation inhibitors.
HAART (Highly Active Antiretroviral Therapy): Combination therapy to prevent resistance.
Additional info: This guide provides a comprehensive overview of immune system disorders relevant to microbiology, integrating mechanisms, clinical features, and therapeutic approaches. For further detail, consult the referenced textbook chapters and tables.
