 Back
BackDisorders Associated with the Immune System: Hypersensitivity, Autoimmunity, Transplantation, Immunodeficiencies, and AIDS
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Disorders Associated with the Immune System
Introduction
The immune system is essential for defending the body against pathogens, but it can also malfunction, leading to disorders such as hypersensitivity, autoimmune diseases, transplant rejection, immunodeficiencies, and acquired immunodeficiency syndrome (AIDS). This chapter explores the mechanisms, examples, and clinical implications of these immune-related disorders.
Hypersensitivity
Definition and Overview
Hypersensitivity refers to an antigenic response that results in undesirable effects, occurring when an individual is sensitized by previous exposure to an antigen (allergen). There are four main types of hypersensitivity reactions, each with distinct mechanisms and clinical manifestations. The study of these reactions is called immunopathology.
Type I (Anaphylactic)
Type II (Cytotoxic)
Type III (Immune Complex)
Type IV (Delayed Cell-Mediated)
The hygiene hypothesis suggests that limiting exposure to pathogens may lower immune tolerance and the ability to cope with harmless antigens, potentially increasing allergies and autoimmune diseases.
Table: Types of Hypersensitivity
Type | Time Before Clinical Signs | Characteristics | Examples |
|---|---|---|---|
I (Anaphylactic) | < 30 min | IgE binds to mast cells or basophils; allergen binding causes degranulation and release of mediators (e.g., histamine). | Anaphylactic shock, hay fever, asthma |
II (Cytotoxic) | 5–12 hours | IgM/IgG antibodies bind to target cell, activate complement, and destroy cell. | Transfusion reactions, Rh incompatibility |
III (Immune Complex) | 3–8 hours | Antigen-antibody complexes cause damaging inflammation. | Serum sickness, rheumatoid arthritis |
IV (Delayed Cell-Mediated) | 24–48 hours | Antigens activate cytotoxic T lymphocytes (CTLs) that kill target cells. | Contact dermatitis, transplant rejection |
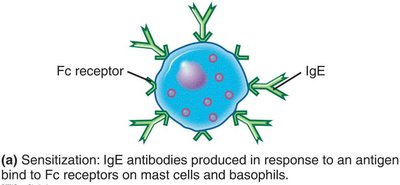
Type I (Anaphylactic) Reactions
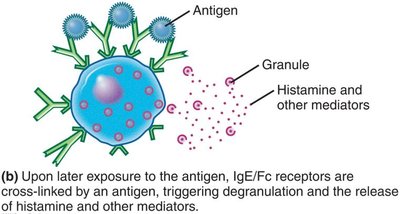
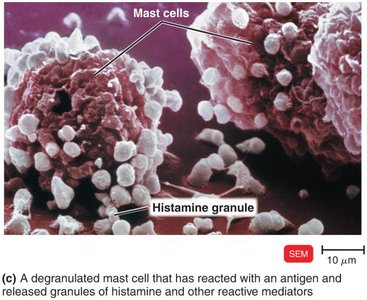
Type I reactions occur within minutes after re-exposure to an allergen. IgE antibodies produced in response to the allergen bind to Fc receptors on mast cells and basophils. Upon subsequent exposure, the allergen cross-links the IgE, triggering degranulation and release of mediators such as histamine, leukotrienes, and prostaglandins.
Histamine: Increases blood vessel permeability.
Leukotrienes: Cause prolonged smooth muscle contraction.
Prostaglandins: Affect smooth muscle and increase mucus secretion.
Systemic vs. Localized Anaphylaxis
Systemic anaphylaxis (anaphylactic shock): Life-threatening, involves cardiovascular and respiratory systems, treated with epinephrine.
Localized anaphylaxis: Limited to specific tissues (e.g., hay fever, asthma), symptoms depend on route of entry.

Food Allergies
Common triggers: eggs, peanuts, tree nuts, milk, soy, fish, wheat, sesame, peas, sulfites.
Symptoms: hives, gastrointestinal upset, possible systemic anaphylaxis.
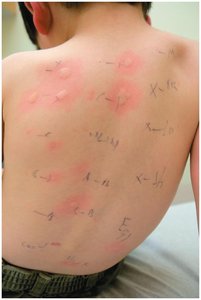
Prevention and Diagnosis
Allergy testing: Skin tests for rapid inflammatory reaction (wheal).
Desensitization: Repeated exposure to increasing antigen doses to induce IgG blocking antibodies.
Type II (Cytotoxic) Reactions
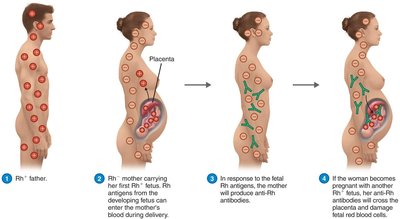
Type II reactions involve IgG or IgM antibodies binding to antigens on cell surfaces, activating complement, and causing cell lysis or damage. Examples include transfusion reactions and hemolytic disease of the newborn (HDNB).
ABO blood group system: Antibodies form against A and/or B antigens on red blood cells (RBCs).
Rh blood group system: Rh-negative mothers can develop anti-Rh antibodies after exposure to Rh-positive fetal blood, risking HDNB in subsequent pregnancies.
Drug-Induced Cytotoxic Reactions
Immune thrombocytopenic purpura: Platelets bind drugs, become antigenic, and are destroyed by antibodies and complement.
Agranulocytosis: Immune destruction of granulocytes.
Hemolytic anemia: Immune destruction of RBCs.

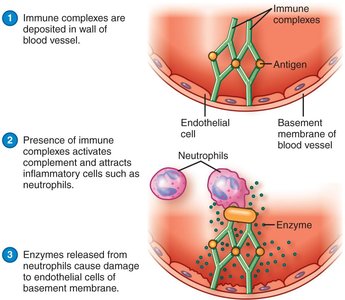
Type III (Immune Complex) Reactions
Type III reactions occur when antibodies form complexes with soluble antigens, which deposit in tissues and activate complement, causing inflammation and tissue damage. The reaction depends on the ratio of antigen to antibody.
Examples: Arthus reaction (rare vaccine side effect), serum sickness, rheumatoid arthritis.
Type IV (Delayed Cell-Mediated) Reactions
Type IV reactions are mediated by T cells and occur 24–48 hours after antigen exposure. Sensitization occurs on first exposure; re-exposure leads to cytokine release and tissue damage.
Examples: Tuberculin skin test, allergic contact dermatitis (e.g., poison ivy, latex, metals).


Autoimmune Diseases
Overview and Mechanisms
Autoimmune diseases occur when the immune system attacks self-antigens, causing organ or tissue damage. Self-tolerance is normally maintained by clonal deletion of self-reactive T cells in the thymus. Loss of self-tolerance leads to autoimmunity, which can be cytotoxic, immune complex-mediated, or cell-mediated.
Examples of Autoimmune Diseases
Cytotoxic: Multiple sclerosis (attack on myelin sheath)
Immune complex: Systemic lupus erythematosus (antibodies against DNA), rheumatoid arthritis (immune complexes in joints)
Cell-mediated: Type 1 diabetes (T cell destruction of pancreatic cells), psoriasis
Autoimmune Disease | Possible Cause |
|---|---|
Rheumatoid arthritis | Immune complexes accumulate in joints |
Systemic lupus erythematosus | Immune complexes involving antibodies against DNA |
Multiple sclerosis | T cells and macrophages attack the myelin sheath |
Type 1 diabetes | T cells destroy insulin-secreting cells |
Graves' disease | Antibodies stimulate thyroid hormone production |
Myasthenia gravis | Antibodies block acetylcholine receptors |
Reactions to Transplantation
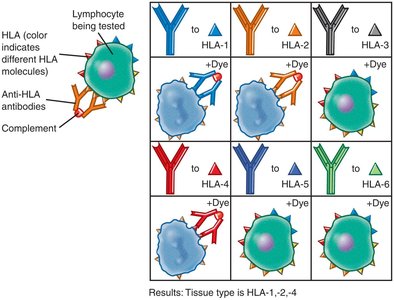
HLA Complex and Tissue Typing
The human leukocyte antigen (HLA) complex is the human version of the major histocompatibility complex (MHC), encoding self-antigens on cell surfaces. HLA typing is crucial for matching donors and recipients in transplantation to reduce rejection risk.
Types of Grafts
Autograft: From self
Isograft: From identical twin
Allograft: From another person
Xenotransplantation: From another species
Privileged Sites and Tissues
Some sites (e.g., cornea) and tissues (e.g., decellularized heart valves) do not provoke immune responses.
Stem Cells in Transplantation
Stem cells are undifferentiated cells capable of generating specialized tissues. Embryonic stem cells are pluripotent, while adult stem cells are multipotent. They are used to regenerate tissues and organs.

Bone Marrow Transplants and Graft-versus-Host Disease
Bone marrow transplants (hematopoietic stem cell transplants) can result in graft-versus-host disease (GVHD) if donor immune cells attack the recipient.
Umbilical cord blood is a less stringent source of stem cells.
Immunosuppression
Immunosuppressive drugs (e.g., cyclosporine, tacrolimus, sirolimus, mycophenolate, basiliximab) are used to prevent transplant rejection by targeting cytokines such as IL-2.
The Immune System and Cancer
Immune Surveillance and Evasion
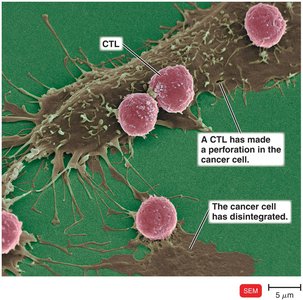
The immune system can recognize and destroy cancer cells via cytotoxic T lymphocytes (CTLs), macrophages, and natural killer (NK) cells. However, cancer cells may evade detection by lacking antigenic epitopes, reproducing rapidly, or becoming invisible to the immune system.
Immunotherapy
Bacterial endotoxins (Coley's toxins) stimulate TNF-α to interfere with tumor blood supply.
Vaccines (e.g., HPV, hepatitis B) prevent virus-associated cancers.
Monoclonal antibodies (e.g., Herceptin) and immunotoxins target cancer cells.
Immunodeficiencies
Types and Examples
Immunodeficiencies are characterized by insufficient immune responses. They can be congenital (genetic, present from birth) or acquired (develop during life due to infections, drugs, or cancers).
Congenital: DiGeorge syndrome (thymic aplasia), SCID, Bruton’s agammaglobulinemia
Acquired: AIDS (caused by HIV), immunosuppression from drugs or cancer
Acquired Immunodeficiency Syndrome (AIDS)
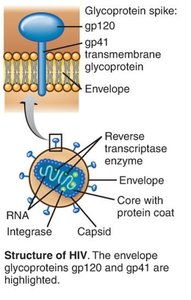
Origin and Structure of HIV
HIV is a retrovirus of the genus Lentivirus with two identical +ssRNA genomes, reverse transcriptase, integrase, and a phospholipid envelope with gp120 spikes. It originated from SIV in chimpanzees in Africa.
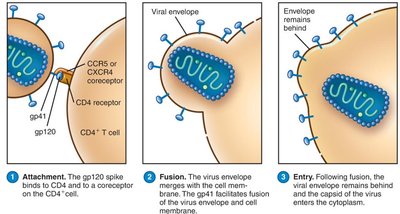
HIV Infection and Pathogenesis
HIV attaches to CD4 receptors (on T helper cells, macrophages, dendritic cells) and coreceptors (CCR5 or CXCR4).
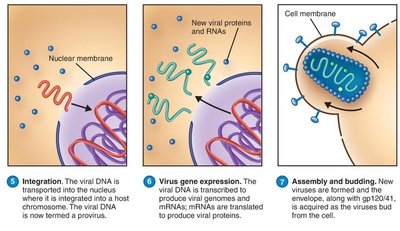
Viral RNA is reverse transcribed to DNA, integrated into host genome (provirus), and may remain latent or actively produce new viruses.
HIV evades immunity by latency, cell-to-cell fusion, and rapid mutation.
Stages of HIV Infection
Phase 1: Acute infection, high viral load, asymptomatic or lymphadenopathy.
Phase 2: Declining CD4+ T cells, persistent infections, few symptoms.
Phase 3 (AIDS): CD4+ T cell count < 200/μL, severe immunodeficiency, opportunistic infections and cancers.
Diseases Associated with AIDS
Pathogen/Disease | Description |
|---|---|
Cryptosporidium hominis | Persistent diarrhea |
Toxoplasma gondii | Encephalitis |
Pneumocystis jirovecii | Life-threatening pneumonia |
Kaposi’s sarcoma | Cancer of skin and blood vessels (HHV-8) |
Diagnosis, Transmission, and Prevention of HIV
Diagnosis: Antibody tests (ELISA, Western blot), nucleic acid amplification tests (NAATs) for HIV RNA.
Transmission: Sexual contact, blood, breast milk, transplacental, needles, organ transplants.
Prevention: Safe sex, needle programs, antiretroviral therapy (ART), PrEP, PEP.
Treatment of HIV/AIDS
Highly Active Antiretroviral Therapy (HAART): Combines drugs targeting different stages of HIV life cycle to minimize resistance.
Drug classes:
Entry inhibitors (e.g., enfuvirtide, maraviroc)
Reverse transcriptase inhibitors (e.g., emtricitabine, tenofovir)
Integrase inhibitors (e.g., raltegravir, dolutegravir)
Protease inhibitors (e.g., atazanavir, indinavir)
Maturation inhibitors, tetherins
Challenges in HIV Vaccine Development
No natural immunity model
Lack of suitable animal models
High mutation rate and immune evasion by HIV
Ideal vaccine would induce CTL response and prevent establishment of latent reservoirs
