 Back
BackDisorders Associated with the Immune System: Hypersensitivity, Autoimmunity, and HIV/AIDS
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Disorders Associated with the Immune System
The Hygiene Hypothesis and Dysbiosis
The hygiene hypothesis proposes that reduced exposure to microbes in early life may lead to increased susceptibility to immune disorders. Dysbiosis, an imbalance in the normal microbiota, can cause adverse effects such as inflammatory bowel diseases (IBDs) and allergies.
Dysbiosis: Disruption of normal gut microbiota, often due to antibiotic therapy, can allow Clostridioides difficile to proliferate, leading to infection.
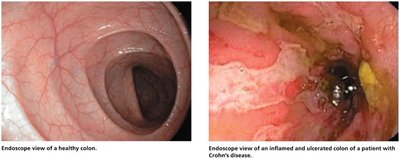
Inflammatory Bowel Diseases (IBDs): Conditions like ulcerative colitis and Crohn’s disease may be linked to dysbiosis.
Allergies and Asthma: Fewer allergies are observed in populations with greater microbial exposure, such as children on farms, compared to urban children.
Treatments: Fecal transplants restore healthy microbiota; whipworm eggs are used experimentally to suppress immune responses in Crohn’s disease.
Example: Fecal transplants and whipworm eggs are used to treat C. difficile infections and Crohn’s disease, respectively.

Hypersensitivity Reactions
Overview of Hypersensitivity
Hypersensitivity is an exaggerated immune response to an antigen, often following prior sensitization. There are four main types, each with distinct mechanisms and clinical manifestations.
Definition: Antigenic response beyond normal, often to harmless antigens (allergens).
Types: Anaphylactic (Type I), Cytotoxic (Type II), Immune Complex (Type III), Delayed Cell-Mediated (Type IV).
Immunopathology: The study of hypersensitivity reactions.
Hygiene Hypothesis: Suggests reduced pathogen exposure lowers immune tolerance.
Type I (Anaphylactic) Reactions
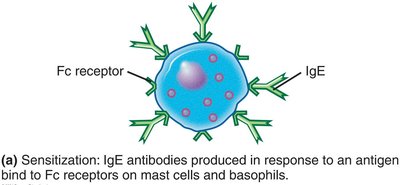
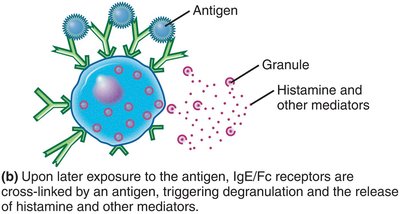
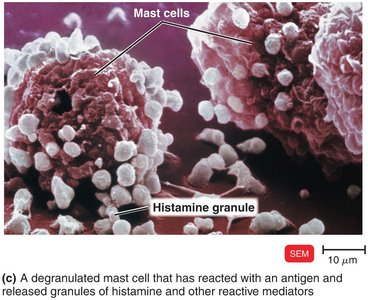
Type I reactions occur within minutes of re-exposure to an allergen. IgE antibodies bind to mast cells and basophils, triggering degranulation and release of mediators such as histamine, leukotrienes, and prostaglandins.
Mechanism: IgE binds to Fc receptors on mast cells/basophils; antigen cross-links IgE, causing degranulation.
Mediators: Histamine increases capillary permeability; leukotrienes cause smooth muscle contraction; prostaglandins increase mucus secretion.
Systemic Anaphylaxis: Severe, rapid reaction affecting cardiovascular and respiratory systems; treated with epinephrine.
Localized Anaphylaxis: Less severe, affects specific tissues (e.g., hay fever, asthma).
Common Allergens: Pollen, dust mites, animal dander, nuts, seafood.

Preventing Anaphylactic Reactions
Allergy testing and desensitization are used to prevent or reduce anaphylactic reactions.
Allergy Testing: Antigens are injected beneath the skin to test for rapid inflammatory response.
Desensitization: Gradual increase in antigen exposure induces IgG production, which blocks allergens.
Type II (Cytotoxic) Reactions
Type II reactions involve IgG or IgM antibodies binding to antigens on cells, activating complement and causing cell lysis or damage. This is exemplified by blood group incompatibilities.
Mechanism: Antibody-antigen binding activates complement, leading to cell destruction.
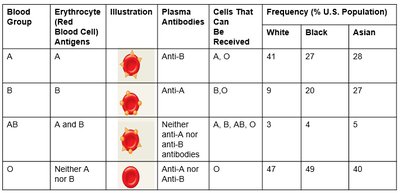
ABO Blood Group System: Antibodies form against carbohydrate antigens on RBCs; transfusion reactions occur if incompatible blood is given.
Rh Blood Group System: Rh+ antigen on RBCs; Rh− individuals can develop anti-Rh antibodies, leading to hemolytic disease of the newborn (HDNB).
Prevention: RhoGAM® administered to Rh− mothers prevents HDNB.
Blood Group | Erythrocyte Antigens | Plasma Antibodies | Cells That Can Be Received | Frequency (% U.S. Population) |
|---|---|---|---|---|
A | A | Anti-B | A, O | White: 41, Black: 27, Asian: 28 |
B | B | Anti-A | B, O | White: 9, Black: 20, Asian: 27 |
AB | A and B | Neither anti-A nor anti-B | A, B, AB, O | White: 3, Black: 4, Asian: 5 |
O | Neither A nor B | Anti-A nor anti-B | O | White: 47, Black: 49, Asian: 40 |
Type III (Immune Complex) Reactions
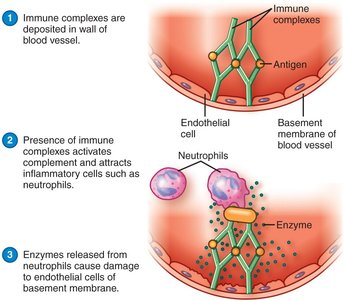
Type III reactions occur when antibodies bind to soluble antigens, forming immune complexes that deposit in tissues and activate complement, causing inflammation and tissue damage.
Mechanism: Immune complexes lodge in basement membranes, activate complement, attract neutrophils, and cause tissue damage.
Examples: Arthus reaction (rare vaccine side effect), serum sickness (reaction to foreign serum).
Type IV (Delayed Cell-Mediated) Reactions
Type IV reactions are mediated by T cells and occur hours to days after antigen exposure. Sensitization involves antigen presentation to T cells; re-exposure triggers cytokine release and inflammation.
Mechanism: Antigen is phagocytized and presented to T cells; memory T cells release cytokines upon re-exposure.
Examples: Tuberculosis skin test, allergic contact dermatitis (e.g., poison ivy, cosmetics, metals, latex).


Autoimmune Diseases
Mechanisms and Examples
Autoimmune diseases occur when the immune system attacks self-antigens, leading to organ damage. Loss of self-tolerance is central to autoimmunity.
Self-Tolerance: Normally maintained by clonal deletion of self-reactive T cells in the thymus.
Autoimmunity: Loss of self-tolerance; can be cytotoxic, immune complex, or cell-mediated.
Prevalence: 80% of autoimmune diseases occur in women.
Immunodeficiencies
Congenital and Acquired Immunodeficiencies
Immunodeficiencies are characterized by insufficient immune responses. They may be congenital (genetic) or acquired (developed during life).
Congenital: Due to defective or missing genes; e.g., DiGeorge syndrome (lack of thymus).
Acquired: Result from drugs, cancers, or infections.
Acquired Immunodeficiency Syndrome (AIDS) and HIV
Origin and Structure of HIV
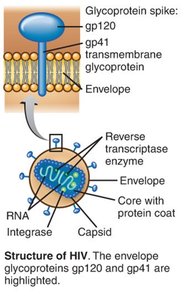
HIV is a retrovirus of the genus Lentivirus, originating from SIV in chimpanzees. It infects T helper cells and is characterized by a phospholipid envelope and glycoprotein spikes (gp120).
Structure: Two identical +RNA molecules, reverse transcriptase, integrase, envelope, gp120 spikes.
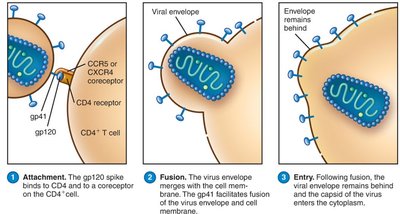
Attachment: gp120 binds to CD4 and a coreceptor on T cells.
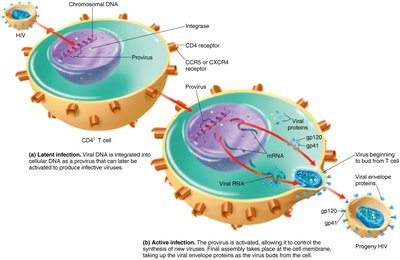
HIV Infectiveness and Pathogenicity
HIV integrates its DNA into host chromosomes, establishing latent and active infections. It evades immune detection through latency, cell-cell fusion, and rapid mutation.
Latent Infection: Viral DNA is hidden as a provirus in host chromosomes.
Active Infection: New viruses bud from host cells.
Immune Evasion: Latency, cell-cell fusion, antigenic variation.
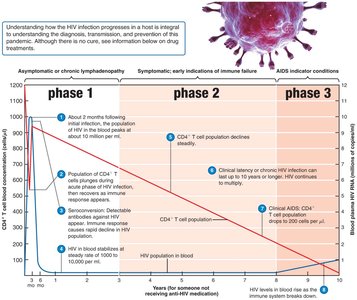
Progression of HIV Infection
HIV infection progresses through three phases: asymptomatic, symptomatic, and AIDS. CD4+ T cell counts decline, leading to immune failure.
Phase 1: Initial strong immune response; CTLs suppress virus.
Phase 2: CD4+ T cell population declines.
Phase 3: AIDS indicator conditions; CD4+ T cell count drops below 200 cells/μL.
Diagnostic Methods for HIV
HIV diagnosis involves antibody tests and nucleic acid amplification tests (NAATs). Seroconversion may delay antibody detection; NAATs detect viral RNA earlier.
Antibody Tests: Screening followed by confirmation (e.g., Western blot).
NAATs: Real-time PCR detects HIV RNA 10–15 days post-exposure.
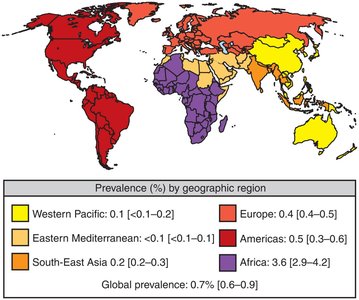
HIV Transmission and Epidemiology
HIV is transmitted via infected cells and body fluids, with blood and semen being most infective. Transmission routes include sexual contact, breast milk, transplacental infection, contaminated needles, organ transplants, and blood transfusions.
Global Prevalence: 36 million infected worldwide; highest rates in Africa.
Most Common Transmission: Heterosexual contact.
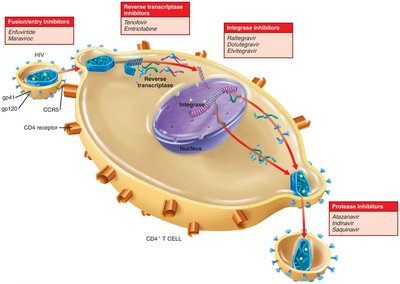
Preventing and Treating AIDS
AIDS is now considered a treatable chronic disease in developed countries. Prevention and treatment strategies include biomedical, behavioral, and structural interventions, as well as antiretroviral therapies.
HAART: Highly active antiretroviral therapy uses multiple drugs to minimize resistance.
PrEP: Preexposure prophylaxis for high-risk individuals.
PEP: Postexposure prophylaxis after potential exposure.
Drug Classes: Fusion/entry inhibitors, reverse transcriptase inhibitors, integrase inhibitors, protease inhibitors.
Challenges in HIV Vaccine Development
Developing an HIV vaccine is difficult due to lack of natural immunity models, high mutation rates, and immune evasion by the virus. An ideal vaccine would induce immunity before latent reservoirs are established and stimulate cytotoxic T lymphocyte (CTL) production.
Obstacles: No natural immunity model, lack of research animals, antigenic invisibility, high mutation rate.
Ideal Vaccine: Induces immunity early, stimulates CTLs, affordable.
