 Back
BackChapter 19Disorders of the Immune System
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Disorders of the Immune System
Overview of Immune System Disorders
The immune system protects the body from pathogens, but failures or malfunctions can lead to disease. Disorders include immunosuppression, hypersensitivity reactions, autoimmunity, and complications related to transplantation and cancer. Understanding these disorders is crucial for diagnosing and treating immune-related diseases.
Immunosuppression: Failure of the immune system to respond adequately to infections or malignancies.
Hypersensitivity: Excessive or inappropriate immune responses to antigens, resulting in tissue damage.
Autoimmunity: Loss of self-tolerance, leading to immune attack on the body's own tissues.
Transplantation Reactions: Immune responses against transplanted tissues or organs.
Cancer Immunology: Immune system interactions with tumor cells, including immune evasion and immunotherapy.
Hypersensitivity Reactions
Classification of Hypersensitivity
Hypersensitivity reactions are classified into four types based on the immune mechanisms involved and the timing of the response. These reactions can be harmful and are often triggered by allergens or foreign antigens.
Type I (Immediate, IgE-mediated): Rapid allergic reactions involving IgE antibodies and mast cells/basophils.
Type II (Antibody-mediated, Cytotoxic): IgG or IgM antibodies target cell-surface antigens, leading to cell destruction.
Type III (Immune Complex-mediated): Antigen-antibody complexes deposit in tissues, causing inflammation.
Type IV (Delayed, T cell-mediated): T cells mediate tissue damage, typically 48–72 hours after exposure.
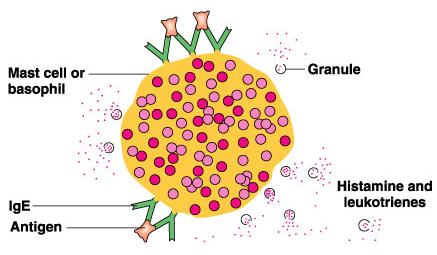
Type I (Immediate, IgE-mediated) Hypersensitivity
Type I hypersensitivity involves the crosslinking of IgE antibodies on mast cells or basophils by soluble allergens, leading to rapid degranulation and release of mediators such as histamine and leukotrienes. This results in symptoms like hives, asthma, or anaphylaxis.
Mechanism: Allergen binds to IgE on mast cells/basophils, causing degranulation.
Symptoms: Localized (e.g., hives, asthma) or systemic (anaphylaxis).
Diagnosis: Skin testing for allergen sensitivity.
Treatment: Desensitization therapy and antihistamines.

Type II (Antibody-mediated, Cytotoxic) Hypersensitivity
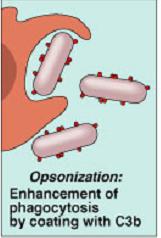
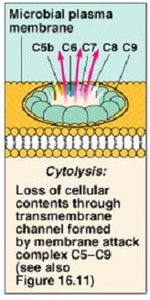
Type II reactions involve IgG or IgM antibodies binding to antigens on cell surfaces, leading to complement activation and cell lysis. This is commonly seen in blood transfusion reactions and certain autoimmune diseases.
Mechanism: Antibody binds to cell-surface antigen, activates complement, and causes cell destruction.
Examples: ABO blood group incompatibility, hemolytic disease of the newborn, drug-induced thrombocytopenic purpura.

ABO Blood Group System
The ABO system is based on the presence of A and B antigens on red blood cells. Individuals produce antibodies against antigens not present on their own cells, leading to transfusion reactions if mismatched blood is given.
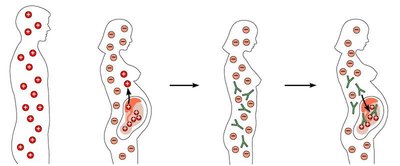
Rh Factor and Hemolytic Disease of the Newborn
Rh incompatibility occurs when an Rh-negative mother is exposed to Rh-positive fetal blood, leading to the production of anti-Rh antibodies. In subsequent pregnancies, these antibodies can attack fetal red blood cells, causing hemolytic disease of the newborn.
Drug-induced Thrombocytopenic Purpura
Certain drugs can bind to platelets, forming complexes that are recognized as foreign by the immune system. Antibody binding and complement activation lead to platelet destruction and hemorrhagic symptoms (purpura).

Type III (Immune Complex-mediated) Hypersensitivity
Type III reactions occur when antigen-antibody complexes form in circulation and deposit in tissues, triggering complement activation and inflammation. This can lead to tissue damage and diseases such as serum sickness and certain forms of glomerulonephritis.
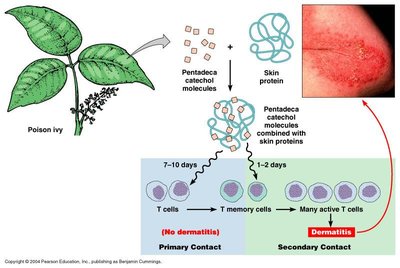
Type IV (Delayed, T cell-mediated) Hypersensitivity
Type IV hypersensitivity is mediated by T cells rather than antibodies. Upon re-exposure to an antigen, memory T cells mount a strong response, recruiting macrophages and causing tissue damage. This reaction is delayed, typically appearing 48–72 hours after exposure.
Examples: Contact dermatitis (e.g., poison ivy), tuberculin skin test, graft rejection.
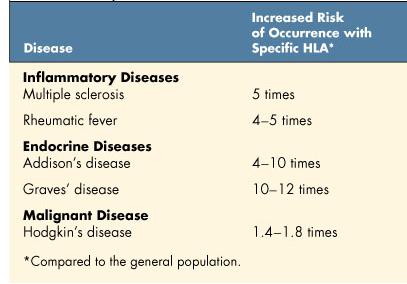
Autoimmune Diseases
Loss of Self-Tolerance
Autoimmunity arises when the immune system fails to distinguish self from non-self, attacking the body's own tissues. Normally, clonal deletion during fetal development eliminates self-reactive T and B cells, but failures in this process can lead to autoimmune diseases.
Examples: Multiple sclerosis, rheumatoid arthritis, type 1 diabetes.
Immune Reactions to Tissue Grafts
Types of Grafts
Autograft: Tissue from the same individual.
Isograft: Tissue from an identical twin.
Allograft: Tissue from another person.
Xenograft: Tissue from a different species.
Graft-versus-host disease can occur when immunocompetent cells in transplanted bone marrow attack the recipient's tissues.
Major Histocompatibility Complex (MHC) and Human Leukocyte Antigen (HLA)
Transplant rejection is primarily mediated by T cells recognizing foreign MHC (HLA in humans) antigens on donor tissue. Matching donor and recipient HLA types is critical to minimize rejection risk.
Privileged Sites: Certain body sites (e.g., eye, brain, testes) are less likely to elicit immune responses to transplants.
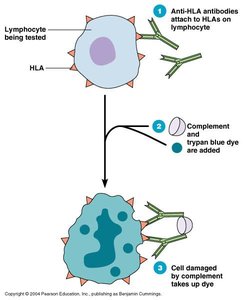
HLA Typing and Immunosuppression
HLA typing can be performed serologically or by gene analysis (PCR) to ensure compatibility. Immunosuppressive drugs are used to prevent graft rejection but increase susceptibility to infections.
Common Drugs: Cyclosporine (suppresses IL-2), mycophenolate mofetil (inhibits T/B cell proliferation), sirolimus (blocks IL-2).
Immune Deficiencies
Types of Immune Deficiencies
Congenital: Genetic defects (e.g., selective IgA deficiency, severe combined immunodeficiency).
Acquired: Result from drugs, cancers, or infections (e.g., HIV/AIDS).
Artificial: Due to immunosuppressive therapy.
Natural: Due to infections such as HIV.
The Immune System and Cancer
Immune Surveillance and Tumor Antigens
Cancer cells may express tumor-specific antigens that can be recognized and destroyed by T cells. However, some cancer cells evade immune detection by lacking antigens or by suppressing immune responses.
Cancer Immunotherapy
Cancer immunotherapy aims to enhance the immune system's ability to recognize and attack cancer cells. Approaches include checkpoint inhibitors, cytokines, cancer vaccines, chimeric antigen receptor (CAR) T cell therapy, monoclonal antibodies, and immunomodulators.
Checkpoint Inhibitors: Block proteins that inhibit T cell activation.
Cytokines: Boost immune cell activity.
Cancer Vaccines: Stimulate immune response against tumor antigens.
CAR T Cell Therapy: Genetically engineered T cells target cancer cells.
Monoclonal Antibodies: Bind to specific antigens on cancer cells.
