 Back
BackChapter 14_Epidemiology and Nosocomial Pathogens
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Principles of Epidemiology
Key Definitions and Concepts
Epidemiology is the study of where and when diseases occur, how they are transmitted, and their impact on populations. Understanding terminology is essential for interpreting epidemiological data and disease dynamics.
Virulence: The ability of a pathogen to overcome host defenses and cause disease.
Disease: A process resulting in tissue damage or change in function/physiology.
Pathogen: An organism or virus capable of causing disease.
Opportunistic Pathogen: Causes disease only in hosts with impaired defenses or in unusual locations.
Pathology: Study of disease.
Etiology: Study of the cause of disease.
Pathogenesis: Development of disease.
Infection: Colonization of the body by pathogens.
Symptom: A change in body function felt by the patient.
Sign: A measurable or observable change in the body.
Syndrome: A specific group of signs and symptoms that accompany a disease.
Types of Diseases
Communicable Disease: Spread from one host to another.
Contagious Disease: Easily spread from one host to another.
Noncommunicable Disease: Not transmitted between hosts.
Frequency and Severity of Disease
Incidence: Fraction of a population that contracts a disease during a specific time (new cases).
Prevalence: Fraction of a population having a specific disease at a given time (all cases).
Sporadic Disease: Occurs occasionally in a population.
Endemic Disease: Constantly present in a population.
Epidemic Disease: Acquired by many hosts in a short time.
Pandemic Disease: Worldwide epidemic.
Herd Immunity: Immunity in most of a population.
Severity and Duration
Acute Disease: Symptoms develop rapidly.
Chronic Disease: Develops slowly, lasts longer.
Subacute Disease: Symptoms between acute and chronic.
Latent Disease: Period of no symptoms when the causative agent is inactive.
Normal Microbiota and the Host
Normal vs. Transient Microbiota
Normal microbiota permanently colonize the host, while transient microbiota are present for limited periods. The distribution and composition of normal microbiota are determined by nutrients, physical and chemical factors, host defenses, and mechanical factors.
Normal Microbiota: Microorganisms that reside permanently in the body.
Transient Microbiota: Microorganisms that are present temporarily.
Human Microbiome Project: Analyzes relationships between microbial communities and human health.

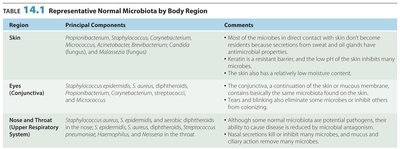
Representative Normal Microbiota by Body Region
Normal microbiota vary by body region and play important roles in health and disease prevention.
Region | Principal Components | Comments |
|---|---|---|
Skin | Propionibacterium, Staphylococcus, Corynebacterium, Micrococcus, Acinetobacter, Brevibacterium, Candida (fungus), Malassezia (fungus) | Most microbes in direct contact with skin do not become residents; secretions from sweat and oil glands have antimicrobial properties. Keratin is a resistant barrier; low moisture content. |
Eyes (Conjunctiva) | Staphylococcus epidermidis, S. aureus, diphtheroids, Propionibacterium, Corynebacterium, Streptococcus, Micrococcus | The conjunctiva is a continuation of the skin or mucous membrane; tears and blinking eliminate some microbes or inhibit others from colonizing. |
Nose and Throat (Upper Respiratory System) | Staphylococcus aureus, S. epidermidis, and aerobic diphtheroids; Streptococcus pneumoniae, Haemophilus, Neisseria | Although some normal microbiota are potential pathogens, they may cause disease if introduced into the sinuses, ears, or lower respiratory tract. Nasal secretions inhibit many microbes; mucus and ciliary action remove many microbes. |
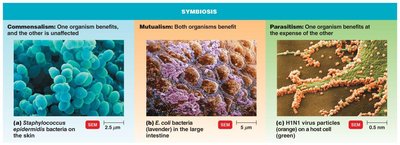
Microbial Antagonism and Symbiosis
Normal microbiota protect the host by competing for nutrients, producing substances harmful to invading microbes, and affecting pH and oxygen availability. Symbiosis describes the relationship between microbiota and the host.
Commensalism: One organism benefits, the other is unaffected.
Mutualism: Both organisms benefit.
Parasitism: One organism benefits at the expense of the other.
Opportunistic Pathogens: Some normal microbiota can cause disease under certain conditions.
Koch’s Postulates and Molecular Postulates
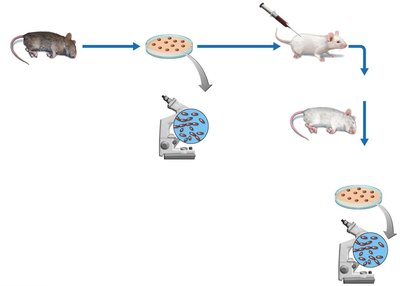
Koch’s Postulates
Koch’s postulates are used to prove the cause of an infectious disease. They involve isolating the pathogen, growing it in pure culture, inoculating a healthy host, and re-isolating the pathogen.
The same pathogen must be present in every case of the disease.
The pathogen must be isolated from the diseased host and grown in pure culture.
The pathogen from the pure culture must cause the disease when inoculated into a healthy, susceptible laboratory animal.
The pathogen must be isolated from the inoculated animal and shown to be the original organism.
Exceptions: Some pathogens cause several disease conditions, some only infect humans, and some microbes have never been cultured.
Molecular Postulates
Virulence factors, resistance genes, plasmids, and transposons contribute to pathogenicity.
Evolutionary aspects: Pathogens may evolve from non-pathogenic forms.
Gene expression and antibody production are important in disease development.
Occurrence and Development of Disease
Incidence and Prevalence
Incidence: Number of people who develop a disease during a particular time period.
Prevalence: Number of people who have a disease at a specified time, including both old and new cases.
Host Predisposing Factors
Immunity (including herd immunity)
Gender (e.g., short urethra in females)
Inherited traits (e.g., sickle cell gene)
Climate and weather
Fatigue, age, lifestyle, chemotherapy
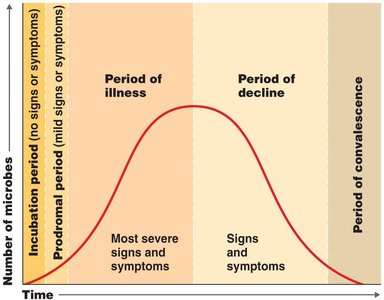
Stages of Disease Development
The progression of disease includes several distinct periods:
Incubation Period: Interval between initial infection and first signs/symptoms.
Prodromal Period: Early, mild symptoms.
Period of Illness: Disease is most severe.
Period of Decline: Signs and symptoms subside.
Period of Convalescence: Body returns to prediseased state.
Reservoirs and Transmission of Disease
Reservoirs of Infection
Reservoirs are continual sources of infection and can be human, animal, or nonliving.
Human Reservoirs: Carriers may have inapparent infections or latent diseases.
Animal Reservoirs: Zoonoses are diseases transmitted from animals to humans (e.g., rabies, Yersinia pestis).
Nonliving Reservoirs: Soil and water (e.g., botulism, tetanus).
Entry and Exit of Pathogens
Respiratory (sneezing)
Contact (skin)
Bodily fluids (blood, saliva, urine)
Diarrhea
Colonization and infection (e.g., bubonic vs. pneumonic plague)
Methods of Disease Transmission
Contact Transmission: Direct, indirect (fomites), and droplet transmission.
Vehicle Transmission: Water, food, air.
Vector Transmission: Arthropods (fleas, ticks, mosquitoes) via mechanical or biological methods.




Healthcare-Associated Infections (HAIs)
Nosocomial Infections
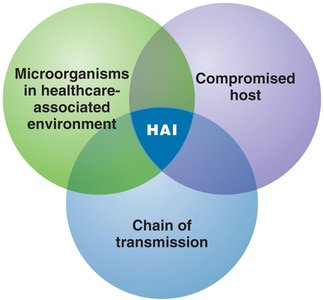
Healthcare-associated infections (HAIs), also known as nosocomial infections, are acquired while receiving treatment in a healthcare facility. They affect a significant proportion of hospital patients and are caused by the interaction of microorganisms, compromised hosts, and chains of transmission.
High density of sick people increases risk.
Common pathogens: Enterococci, Pseudomonas, Staphylococcus species.
Common sites: Urinary tract, surgical wounds, respiratory tract, bloodstream.
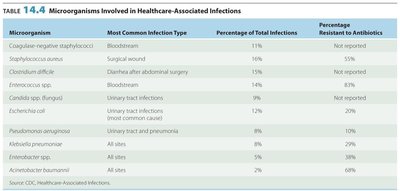
Microorganisms Involved in Healthcare-Associated Infections
Microorganism | Most Common Infection Type | Percentage of Total Infections | Percentage Resistant to Antibiotics |
|---|---|---|---|
Coagulase-negative staphylococci | Bloodstream | 11% | Not reported |
Staphylococcus aureus | Surgical wound | 16% | 55% |
Clostridium difficile | Diarrhea after abdominal surgery | 14% | Not reported |
Enterococcus spp. | Bloodstream | 10% | Not reported |
Candida spp. | Urinary tract infections | 9% | Not reported |
Escherichia coli | Urinary tract infections | 8% | 20% |
Pseudomonas aeruginosa | Urinary tract and pneumonia | 8% | 10% |
Klebsiella pneumoniae | All sites | 8% | 20% |
Acinetobacter baumannii | All sites | 2% | 68% |
Control and Prevention of Nosocomial Infections
Aseptic techniques
Careful handling of contaminated materials
Frequent and thorough handwashing
Education about infection control
Use of isolation rooms and wards
Cleaning and disinfecting equipment
Periodic examination by infection control committees
Epidemiological Investigations and Surveillance
Types of Epidemiological Investigations
Descriptive: Collects data describing disease occurrence (retrospective and prospective).
Analytical: Identifies probable cause (case-control and cohort studies).
Experimental: Tests hypotheses (e.g., drug effectiveness).
Surveillance and Reporting
CDC, WHO, and local health departments monitor and report outbreaks.
CDC publishes Morbidity and Mortality Weekly Report (MMWR).
Foodborne Disease Outbreak Surveillance System collects outbreak data.
Online databases provide public access to outbreak information.
Key Terms
Morbidity Rate: Number of people affected by a disease in a given period relative to the population.
Mortality Rate: Number of deaths resulting from a disease in a given period relative to the population.
Notifiable Infectious Diseases: Diseases that must be reported to public health authorities.
Emerging Infectious Diseases
Definition and Contributing Factors
Emerging infectious diseases are new, increasing in incidence, or have the potential to increase. Factors include genetic recombination, evolution of new strains, inappropriate use of antibiotics, changes in weather, modern transportation, ecological disasters, animal control measures, and public health failures.
Genetic Recombination: e.g., E. coli O157, avian influenza (H5N1)
Evolution of New Strains: e.g., V. cholerae O139
Antibiotic Resistance: Inappropriate use leads to resistant strains.
Weather Changes: e.g., Hantavirus
Modern Transportation: e.g., West Nile virus
Ecological Disaster/War: e.g., Coccidioidomycosis
Animal Control Measures: e.g., Lyme disease
Public Health Failure: e.g., Diphtheria
Summary Table: Disease Transmission Methods
Transmission Method | Description | Example |
|---|---|---|
Direct Contact | Physical contact between infected and susceptible host | Touching, kissing |
Indirect Contact | Via fomites (nonliving objects) | Doorknobs, bedding |
Droplet | Airborne droplets less than 1 meter | Sneezing, coughing |
Vehicle | Transmission by water, food, air | Contaminated water, foodborne illness |
Vector | Arthropods transmit pathogens | Mosquitoes, fleas |
Key Equations
Incidence Rate:
Prevalence Rate:
Morbidity Rate:
Mortality Rate:
Historical Contributions to Epidemiology
John Snow: Mapped cholera occurrence in London (1848–1849).
Ignaz Semmelweis: Demonstrated handwashing reduced puerperal sepsis (1846–1848).
Florence Nightingale: Showed improved sanitation decreased epidemic typhus (1858).
Conclusion
Epidemiology provides the framework for understanding disease occurrence, transmission, and control. Knowledge of normal microbiota, disease development, transmission methods, and healthcare-associated infections is essential for preventing and managing infectious diseases.
