 Back
BackGram-Negative Cocci and Medically Important Spirochetes: Neisseria, Treponema, Borrelia, and Leptospira
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Gram-Negative Cocci
Genus Neisseria
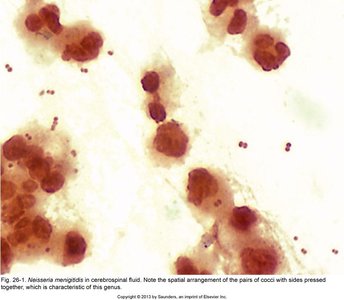
The genus Neisseria includes Gram-negative cocci of major medical importance, particularly Neisseria gonorrhoeae and Neisseria meningitidis. These bacteria are often found in pairs (diplococci) or short chains and are characterized by the absence of flagella, the presence of capsules in pathogenic species, and pili/fimbriae for attachment and conjugation. They are aerobic or microaerophilic, oxidase positive, and most are catalase positive. Pathogenic species require enriched complex media and increased CO2 for growth.
Key Features: Gram-negative, diplococci, oxidase positive, capsule (in pathogens), pili/fimbriae, aerobic/microaerophilic.
Habitat: Some species are normal flora in the oral/respiratory tract, complicating diagnosis.
Neisseria gonorrhoeae: The Gonococcus
Neisseria gonorrhoeae is the causative agent of gonorrhea, a common sexually transmitted infection (STI). It possesses several virulence factors that contribute to its pathogenicity.
Virulence Factors:
Endotoxin (lipooligosaccharide)
Pili: Mediate attachment, conjugation, and resistance to neutrophil phagocytosis
Porin B: Interferes with neutrophil degranulation
IgA protease: Cleaves IgA antibodies
Antigenic variation: Multiple serotypes
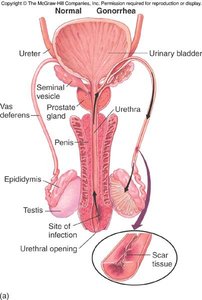
Epidemiology and Pathology of Gonorrhea
Gonorrhea is strictly a human infection and is among the top five STIs globally. It is highly prevalent in young adults and adolescents, with over 500,000 cases reported annually in the US and more than 82 million new cases worldwide each year. The infectious dose is low (100–1,000 organisms in males), and the bacterium does not survive long outside the host.
Transmission: Sexual contact, perinatal (to newborns during birth)
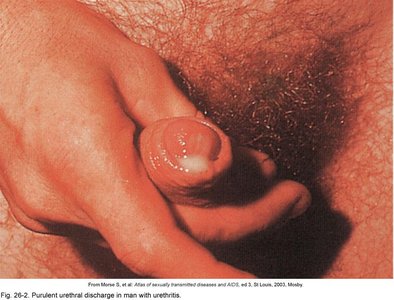
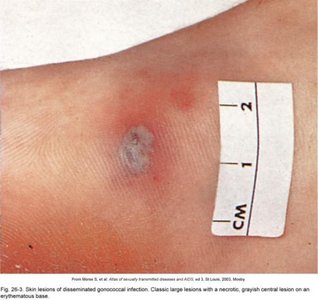
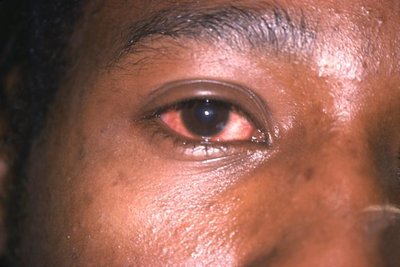
Symptoms in Males: Urethritis, yellowish discharge, scarring, infertility; extragenital infections (anal, oral, conjunctivitis, septicemia, arthritis, skin lesions)
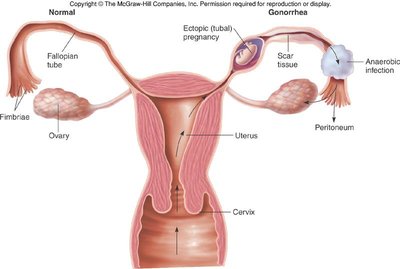
Symptoms in Females: 50% symptomatic (discharge, vaginitis, urethritis, pelvic inflammatory disease), 50% asymptomatic; increased risk of sterility, ectopic pregnancy, and HIV transmission
Extragenital Infections: Similar to males
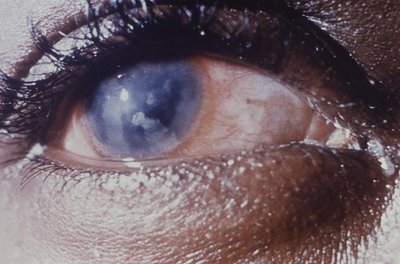
Gonorrhea in Newborns
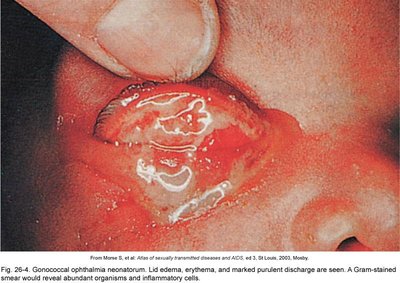
Newborns can acquire gonococcal infection during passage through the birth canal, leading to ophthalmia neonatorum (eye inflammation and potential blindness). Prophylactic eye drops are used for prevention, though shortages have been reported.
Diagnosis and Control of Gonorrhea
Diagnosis:
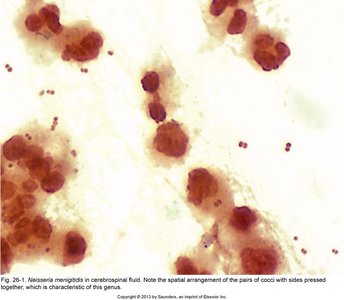
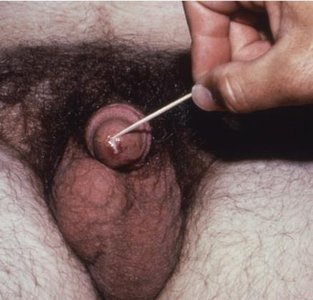
Gram stain: Gram-negative diplococci, often intracellular, from exudate (urethral, vaginal, cervical, or eye)
NAAT (Nucleic Acid Amplification Test): Sensitive but may not distinguish resistance or normal flora
Treatment: Ceftriaxone (3rd generation cephalosporin) is the main reliable therapy; resistance is rising
Prevention: Reportable disease, safe sex practices, prophylaxis for newborns
Neisseria meningitidis: The Meningococcus
Neisseria meningitidis is a leading cause of bacterial meningitis, especially in children and young adults. It is characterized by rapid onset and high mortality if untreated.
Virulence Factors: Capsule, adhesive fimbriae, IgA protease, endotoxin
Serotypes: 12 capsular antigen types; A, B, C, Y, W cause most disease
Reservoir: Human nasopharynx; higher carriage in institutional settings (e.g., dormitories)
Pathogenesis: Bacteria cross the blood-brain barrier, causing meningitis and meningococcemia (sepsis with hemorrhage and petechiae)
Complications: Permanent neurological damage (10–20%), death (10–15%)
Diagnosis, Treatment, and Prevention of Meningococcal Disease
Diagnosis:
Gram stain of CSF or blood
Cultures for differentiation and susceptibility
Oxidase test (positive)
Rapid antigen tests for capsular polysaccharides
Serotyping with specific antibodies
PCR (NAA tests): Detects DNA but not resistance
Treatment: IV or IM 3rd generation cephalosporins; prophylaxis for close contacts
Prevention: Vaccines (conjugate for A, C, W, Y; recombinant protein for B; combination vaccines for high-risk groups)
Medically Important Spirochetes
General Characteristics
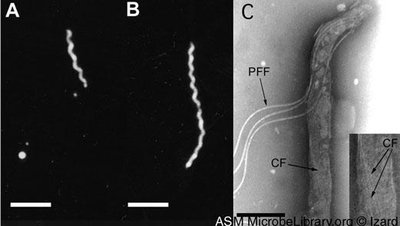
Spirochetes are Gram-negative, spiral-shaped bacteria. Most are saprobes or commensals, but some are important human pathogens. They lack typical LPS in their outer membrane but have lipoproteins. Major genera include Treponema, Borrelia, and Leptospira.
Genus Treponema
Treponema species are thin, regularly coiled cells with periplasmic flagella. They are microaerophilic or anaerobic and are found in the oral cavity, intestinal tract, and perigenital regions. Pathogenic species are strict parasites and require live cells for cultivation.
Metabolism: Some species rely solely on glycolysis for ATP production
Genome: Small, about 1,000 genes
Treponema pallidum subsp. pallidum: Syphilis
Treponema pallidum is the causative agent of syphilis, a chronic, systemic STI. It is microaerophilic, extremely fastidious, and sensitive to environmental conditions. Transmission occurs via sexual contact or transplacentally.
Pathogenesis: Binds to epithelium, multiplies, penetrates capillaries, and disseminates via circulation
Clinical Stages: Primary, secondary, tertiary (late)
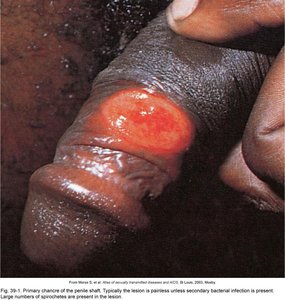
Primary Syphilis
Characterized by a hard, painless chancre at the site of inoculation and regional lymphadenopathy. Incubation is 10–90 days, and the lesion heals spontaneously in 3–6 weeks in about one-third of cases.
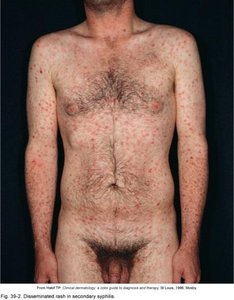
Secondary Syphilis
Known as "the great pretender" due to its varied manifestations. Presents with flu-like symptoms, generalized rash (often on palms and soles), and mucocutaneous lesions (condylomata lata). Rash disappears spontaneously and may enter a latent phase. The Jarisch-Herxheimer reaction (fever, aches) may occur after penicillin treatment.



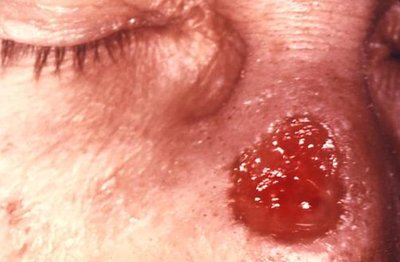
Tertiary (Late) Syphilis
Occurs in about 30% of untreated cases, years to decades after initial infection. Characterized by gummas (necrotic lesions), cardiovascular syphilis (arteritis, aneurysms, heart valve damage), and neurosyphilis (dementia, stroke, seizures, blindness).
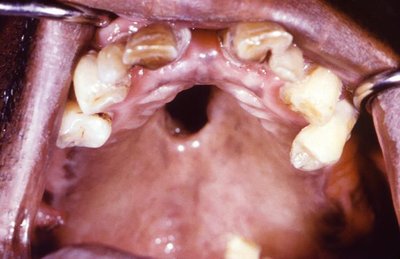

Congenital Syphilis
Transmitted transplacentally, leading to stillbirth, neonatal death, or severe deformities (nasal discharge, skin lesions, bone and teeth abnormalities, "late" syphilis features). Incidence is rising in some regions.




Diagnosis and Treatment of Syphilis
Diagnosis:
Symptoms and history
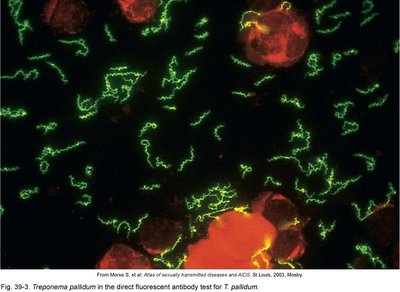
Microscopy: Darkfield or fluorescent antibody staining
Serology: RPR, VDRL (nonspecific); TP-PA, FTA-ABS, EIA, Western blot (specific)
Treatment: Penicillin (Benzathine penicillin for early syphilis; penicillin G for late/tertiary)
Prevention: Safe sex practices, screening, and treatment of pregnant women
Nonsyphilitic Treponematoses
Bejel: Treponema pallidum subsp. endemicum; deforming childhood infection in Middle East/North Africa
Yaws: Treponema pallidum subsp. pertenue; skin and bone lesions, Central Africa/South America/Indonesia
Pinta: Treponema carateum; superficial skin lesions, Central/South America
Treponema denticola
Major contributor to periodontal disease, usually found in biofilms with other organisms. It is anaerobic and produces adhesins, peptidases, and pore-forming proteins that help evade host defenses and degrade host tissues.
Borrelia: Arthropod-Borne Spirochetes
Borrelia species are large, irregularly coiled spirochetes transmitted by arthropod vectors. They stain poorly with Gram stain but can be visualized with special stains.
Relapsing Fever: B. recurrentis (louse-borne), B. hermsii (tick-borne)
Lyme Disease: B. burgdorferi, B. mayonii (Ixodes tick vector)
Lyme Disease
Nonfatal, slowly progressive syndrome. Characterized by erythema migrans (bull's-eye rash), fever, headache, stiff neck, and, if untreated, cardiac, neurological, and arthritic complications. Treated with tetracyclines or beta-lactams. Prevention includes tick avoidance and prompt removal.
Relapsing Fevers
Reservoirs are wild rodents; vectors are ticks or lice. Characterized by recurring fever due to antigenic variation of outer surface proteins. Treated with tetracyclines or penicillins; Jarisch-Herxheimer reaction may occur.
Leptospira
Leptospira species are thin, coiled spirochetes with hooked ends. They are obligate aerobes, require specialized media, and are maintained in small animal reservoirs. Infection occurs via skin contact with contaminated water, leading to endothelial damage and, in severe cases, Weil disease (renal/hepatic dysfunction, vasculitis, myocarditis). Diagnosed by microscopic agglutination test; treated with doxycycline.
Genus | Key Disease(s) | Transmission | Main Features |
|---|---|---|---|
Neisseria gonorrhoeae | Gonorrhea | Sexual, perinatal | Urethritis, PID, conjunctivitis, infertility |
Neisseria meningitidis | Meningitis, meningococcemia | Respiratory droplets | Rapid onset, petechiae, shock |
Treponema pallidum | Syphilis | Sexual, transplacental | Chancre, rash, gummas, neurological |
Borrelia burgdorferi | Lyme disease | Tick bite | Bull's-eye rash, arthritis, carditis |
Leptospira interrogans | Leptospirosis | Contact with animal urine/water | Fever, renal/hepatic dysfunction |
