 Back
BackImmune Deficiency Diseases and Hypersensitivity: Mechanisms, Disorders, and HIV/AIDS
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Immune Deficiency Diseases and Hypersensitivity
Introduction
This study guide covers the mechanisms and clinical implications of immune deficiency diseases and hypersensitivity reactions, including autoimmune disorders, transplantation immunology, and HIV/AIDS. These topics are central to understanding the immune system's role in health and disease, as outlined in microbiology curricula.
Hypersensitivity
Overview of Hypersensitivity
Hypersensitivity refers to an exaggerated immune response to antigens (allergens) that results in tissue damage. There are four main types, each with distinct mechanisms and clinical presentations.
Type I (Anaphylactic): Rapid onset, mediated by IgE antibodies.
Type II (Cytotoxic): Involves IgG or IgM antibodies and complement, leading to cell lysis.
Type III (Immune Complex): Immune complexes deposit in tissues, causing inflammation.
Type IV (Delayed Cell-Mediated): T cell-mediated, with delayed onset.
Hygiene Hypothesis: Suggests that reduced exposure to antigens in overly clean environments lowers immune tolerance, increasing hypersensitivity risk.
Types of Hypersensitivity Reactions
Type of Reaction | Time After Exposure |
|---|---|
Type I (Anaphylactic) | <30 min |
Type II (Cytotoxic) | 5–12 hours |
Type III (Immune Complex) | 3–8 hours |
Type IV (Delayed Cell-Mediated) | ≥1 day |
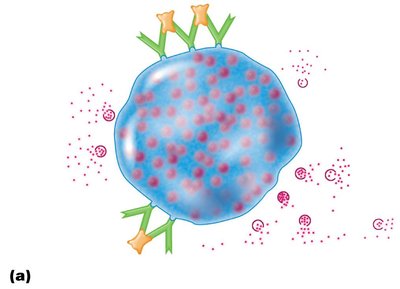
Type I (Anaphylactic) Reactions
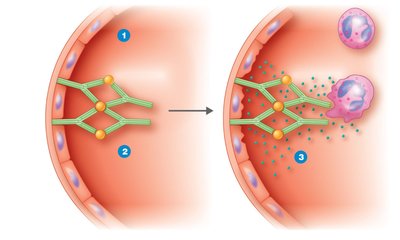
Type I hypersensitivity involves IgE antibodies bound to mast cells and basophils. Upon exposure to the allergen, cross-linking of IgE triggers degranulation and release of mediators such as histamine, leukotrienes, and prostaglandins, leading to allergic symptoms.
Systemic anaphylaxis: Can cause circulatory collapse and death.
Localized anaphylaxis: Includes hives, hay fever, and asthma.

Diagnosis: Skin tests are used to identify specific allergens.
Prevention: Desensitization injections stimulate IgG production, which blocks allergen binding to IgE.
Type II (Cytotoxic) Reactions
Type II reactions involve IgG or IgM antibodies directed against cell surface antigens, activating complement and leading to cell lysis or phagocytosis. Classic examples include transfusion reactions and hemolytic disease of the newborn.
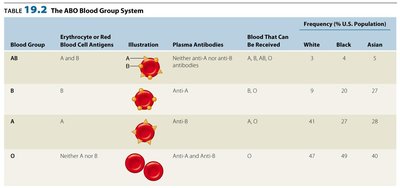
ABO Blood Group System: Incompatibility leads to hemolysis.
Blood Group | Erythrocyte Antigens | Plasma Antibodies | Blood That Can Be Received | Frequency (%) |
|---|---|---|---|---|
AB | A and B | Neither anti-A nor anti-B | AB, A, B, O | White: 4, Black: 4, Asian: 5 |
B | B | Anti-A | B, O | White: 11, Black: 20, Asian: 27 |
A | A | Anti-B | A, O | White: 41, Black: 27, Asian: 28 |
O | Neither A nor B | Anti-A and Anti-B | O | White: 47, Black: 49, Asian: 40 |
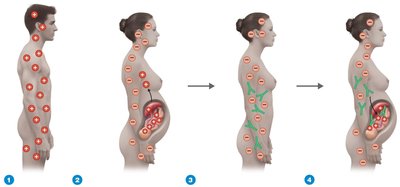
Hemolytic Disease of the Newborn: Occurs when an Rh– mother produces anti-Rh antibodies that attack Rh+ fetal red blood cells in subsequent pregnancies.
Type III (Immune Complex) Reactions
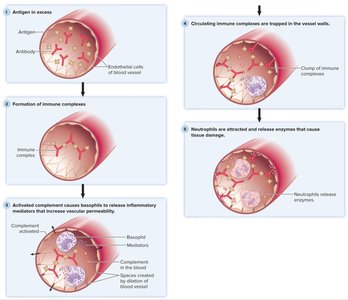
Type III hypersensitivity is mediated by immune complexes (antigen-antibody aggregates) that deposit in tissues, activating complement and attracting neutrophils, which release enzymes causing tissue damage. Examples include systemic lupus erythematosus and glomerulonephritis.
Type IV (Delayed Cell-Mediated) Reactions
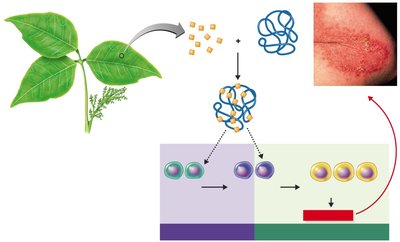
Type IV hypersensitivity is mediated by T cells (especially cytotoxic T lymphocytes, CTLs). The reaction is delayed (24–48 hours) and involves cytokine-mediated recruitment of macrophages and cytotoxic cells, leading to tissue damage. Examples include allergic contact dermatitis (e.g., poison ivy) and latex allergy.

Autoimmune Diseases
Mechanisms and Types
Autoimmunity is the loss of self-tolerance, leading to immune responses against the body's own tissues. Mechanisms include:
Cytotoxic: Antibodies react with cell-surface antigens (e.g., Graves’ disease).
Immune Complex: Immune complexes deposit in tissues (e.g., systemic lupus erythematosus).
Cell-Mediated: T cell-mediated tissue damage (e.g., psoriasis).
Clonal deletion during fetal development normally ensures self-tolerance.
Transplantation Immunology
HLA and Graft Types
Histocompatibility antigens (encoded by the major histocompatibility complex, MHC, or HLA in humans) are critical for tissue compatibility. Tissue typing is used to match donor and recipient HLAs to minimize rejection.

Autograft: Self-tissue
Isograft: Identical twin
Allograft: Another person
Xenograft: Nonhuman tissue
Immunosuppression is required to prevent rejection, using drugs such as cyclosporine, tacrolimus, and others that inhibit T cell activation.
The Immune System and Cancer
Immune Surveillance and Immunotherapy
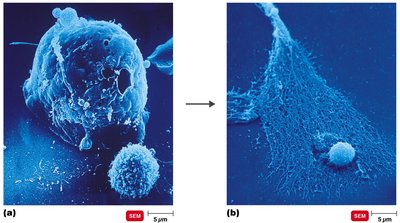
Cancer cells express tumor-associated antigens and are targeted by cytotoxic T lymphocytes (CTLs). Immunotherapies include monoclonal antibodies, cytokines (e.g., TNF, IL-2), and vaccines targeting tumor antigens.
Immunodeficiencies
Types and Examples
Immunodeficiencies are conditions where the immune system is impaired. They can be:
Congenital: Genetic defects (e.g., severe combined immunodeficiency, SCID).
Acquired: Result from infections (e.g., HIV), drugs, or cancers.
Disease | Cells Affected |
|---|---|
AIDS | TH (CD4+) cells |
Selective IgA immunodeficiency | B, T cells |
Common variable hypogammaglobulinemia | B, T cells (decreased immunoglobulins) |
Reticular dysgenesis | B, T, and stem cells |
Severe combined immunodeficiency | B, T, and stem cells |
Thymic aplasia (DiGeorge syndrome) | T cells (defective thymus) |
Wiskott-Aldrich syndrome | B, T cells |
X-linked infantile (Bruton’s) agammaglobulinemia | B cells (decreased immunoglobulins) |
HIV/AIDS
HIV Structure and Infection Mechanism
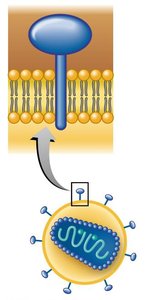
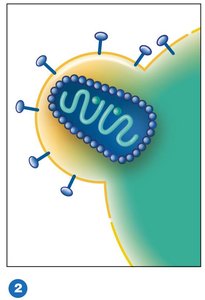
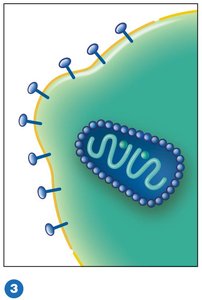
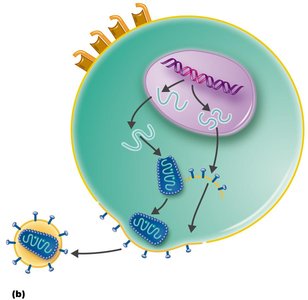
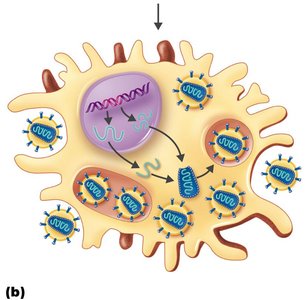
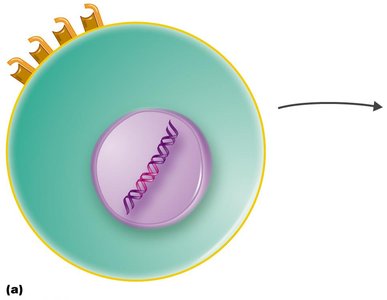
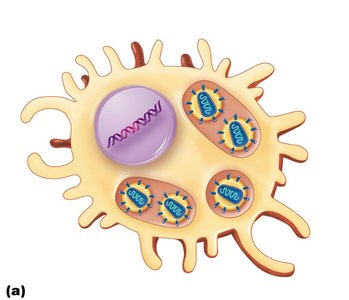
HIV is a retrovirus that infects CD4+ T cells, leading to acquired immunodeficiency syndrome (AIDS). The virus attaches to CD4 and coreceptors (CCR5 or CXCR4), fuses with the cell membrane, and releases its RNA genome, which is reverse transcribed and integrated into the host genome as a provirus.

HIV Replication and Latency
After integration, HIV can remain latent or become active, producing new virions that bud from the host cell. Latency allows the virus to evade immune detection and antiretroviral drugs.
HIV Types and Global Distribution
HIV-1: Main type, with subtypes (clades) B, C, E, etc.
HIV-2: Less common, mainly in West Africa.
Clinical Stages of HIV Infection
Phase 1: Asymptomatic or chronic lymphadenopathy.
Phase 2: Symptomatic, early immune failure.
Phase 3: AIDS-defining conditions (e.g., opportunistic infections).
Diagnosis and Transmission
Diagnosis: ELISA for antibodies, Western blot, PCR for viral RNA.
Transmission: Sexual contact, blood, perinatal, breast milk, contaminated needles.
Prevention and Treatment
Prevention: Safe sex, sterile needles, universal precautions for healthcare workers.
Antiretroviral Therapy (ART): Includes reverse transcriptase inhibitors, protease inhibitors, entry inhibitors, and integrase inhibitors.
HAART (Highly Active Antiretroviral Therapy): Combination of drugs to suppress viral replication and delay progression to AIDS.
Vaccine development is challenging due to HIV's high mutation rate, clade diversity, and latent reservoirs.
Summary Table: Types of Hypersensitivity
Type | Immune Mechanism | Example |
|---|---|---|
I (Anaphylactic) | IgE-mediated, mast cell degranulation | Allergic rhinitis, anaphylaxis |
II (Cytotoxic) | IgG/IgM + complement, cell lysis | Transfusion reaction, hemolytic disease of newborn |
III (Immune Complex) | Immune complex deposition, complement activation | Serum sickness, lupus |
IV (Delayed Cell-Mediated) | T cell-mediated, cytokine release | Contact dermatitis, TB skin test |
Additional info: This guide integrates textbook-level explanations and visual aids to reinforce key concepts in immunology, hypersensitivity, autoimmunity, transplantation, and HIV/AIDS for microbiology students.
