 Back
BackImmune Disorders: Hypersensitivities, Autoimmunity, and Immunodeficiency
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Immune Disorders
Overview of Immune Disorders
Immune disorders arise when the immune system malfunctions, leading to exaggerated, insufficient, or misdirected immune responses. These disorders are classified into hypersensitivities, autoimmune diseases, and immunodeficiency diseases. Understanding these categories is essential for recognizing the mechanisms and clinical implications of immune dysfunction.
Hypersensitivities
Definition and Types of Hypersensitivity
Hypersensitivity refers to any immune response against a foreign antigen that is exaggerated beyond the norm. There are four main types, each with distinct mechanisms and clinical manifestations:
Type I (Immediate) – Allergy, mediated by IgE and mast cell degranulation
Type II (Cytotoxic) – Antibody-mediated cell destruction
Type III (Immune Complex-Mediated) – Immune complex deposition and inflammation
Type IV (Delayed or Cell-Mediated) – T cell-mediated tissue damage
Type I (Immediate) Hypersensitivity
Type I hypersensitivity is a rapid, antibody-mediated reaction to allergens, resulting in the release of inflammatory mediators. It is commonly known as an allergy and can be localized or systemic.
Mechanism: Involves two steps: Sensitization (initial exposure to allergen) and Degranulation (release of mediators upon re-exposure).
Key Cells: Mast cells, basophils, and eosinophils play central roles in mediating allergic responses.
Clinical Manifestations: Range from mild (hay fever, hives) to severe (anaphylactic shock).

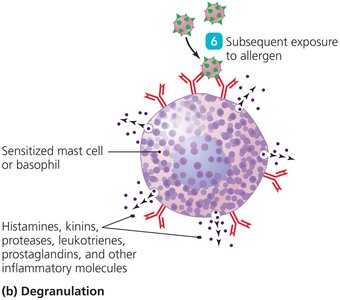
Inflammatory Molecules Released from Mast Cells
Molecule | Role in Hypersensitivity Reactions |
|---|---|
Histamine | Causes smooth muscle contraction, increased vascular permeability, and irritation |
Kinins | Cause smooth muscle contraction, inflammation, and irritation |
Proteases | Damage tissues and activate complement |
Leukotrienes | Cause slow, prolonged smooth muscle contraction, inflammation, and increased vascular permeability |
Prostaglandins | Some contract smooth muscle; others relax it |
Common Allergens and Clinical Signs
Allergens include pollen, fungal spores, dust mites, animal dander, and certain foods.
Localized reactions depend on the portal of entry (e.g., hay fever from inhaled allergens, hives from skin contact).
Systemic reactions can cause anaphylaxis, a life-threatening emergency requiring epinephrine.


Diagnosis, Prevention, and Treatment
Diagnosis: Detection of allergen-specific IgE (e.g., ImmunoCAP test) and skin testing.
Prevention: Avoidance of allergens, elimination diets, and immunotherapy (allergy shots).
Treatment: Antihistamines, glucocorticoids, bronchodilators, and epinephrine for severe reactions.

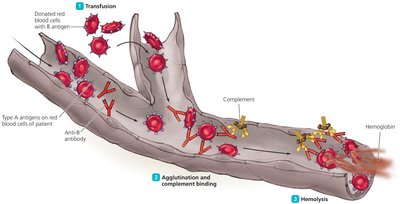
Type II (Cytotoxic) Hypersensitivity
Type II hypersensitivity involves the destruction of cells by antibodies and complement, often seen in blood transfusion reactions and hemolytic disease of the newborn.
Mechanism: Antibodies bind to antigens on cell surfaces, leading to cell lysis via complement activation.
Examples: ABO blood group incompatibility, Rh incompatibility in pregnancy.
ABO Blood Group System
ABO Blood Group | ABO Antigen(s) Present | Antibodies Present | Can Donate To | Can Receive From |
|---|---|---|---|---|
A | A | Anti-B | A or AB | A or O |
B | B | Anti-A | B or AB | B or O |
AB | A and B | None | AB | A, B, AB, or O (universal recipient) |
O | None | Both anti-A and anti-B | A, B, AB, or O (universal donor) | O |
Rh System and Hemolytic Disease of the Newborn
Rh antigen is present in most humans (Rh+).
Rh− mothers carrying Rh+ fetuses may develop antibodies that attack fetal red blood cells in subsequent pregnancies.
Prevention with RhoGAM (anti-Rh immunoglobulin) is effective.

Type III (Immune Complex–Mediated) Hypersensitivity
Type III hypersensitivity is caused by the formation and deposition of immune complexes, which trigger inflammation and tissue damage.
Mechanism: Immune complexes activate complement and attract neutrophils, leading to tissue injury.
Examples: Hypersensitivity pneumonitis, glomerulonephritis, rheumatoid arthritis, systemic lupus erythematosus (SLE).

Clinical Manifestations
Hypersensitivity pneumonitis: Inhaled antigens cause immune complex formation in the lungs.
Glomerulonephritis: Immune complexes deposit in kidney glomeruli, leading to renal failure.
Rheumatoid arthritis: Immune complexes in joints cause chronic inflammation and joint deformity.
Systemic lupus erythematosus (SLE): Autoantibodies against DNA and other cell components cause widespread tissue damage.


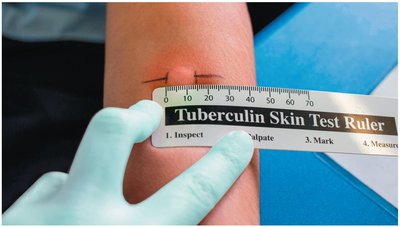
Type IV (Delayed or Cell-Mediated) Hypersensitivity
Type IV hypersensitivity is mediated by T cells and occurs 12–24 hours after antigen exposure. It is characterized by inflammation and tissue damage at the site of antigen contact.
Mechanism: Involves antigen-presenting cells and T cells; delay is due to migration and activation of T cells and macrophages.
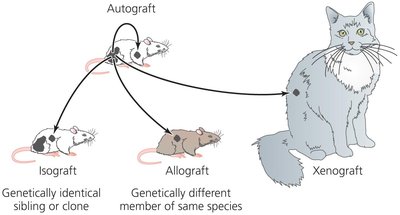
Examples: Tuberculin skin test, allergic contact dermatitis, graft rejection, graft-versus-host disease.

Summary Table: Characteristics of the Four Types of Hypersensitivity
Descriptive Name | Cause | Time Course | Characteristic Cells Involved |
|---|---|---|---|
Immediate (Type I) | IgE on sensitized cells binds antigen, causing degranulation | Seconds to minutes | Mast cells, basophils |
Cytotoxic (Type II) | Antibodies and complement lyse target cells | Minutes to hours | Plasma cells (antibodies) |
Immune Complex-Mediated (Type III) | Antibody-antigen complexes trigger complement, inflammation | Several hours | Neutrophils |
Delayed (Type IV) | T cells attack body cells | Several days | Activated T cells |
Immunosuppressive Drugs in Transplantation
Class | Examples | Action |
|---|---|---|
Glucocorticoids | Prednisone, methylprednisolone | Anti-inflammatory; kill T cells |
Cytotoxic drugs | Cyclophosphamide, azathioprine, etc. | Block cell division nonspecifically |
Cyclosporine | Cyclosporine | Blocks T cell responses |
Lymphocyte-depleting therapies | Antilymphocyte globulin, monoclonal antibodies | Kill T cells nonspecifically or inhibit IL-2 reception |
Autoimmune Diseases
Causes of Autoimmune Diseases
Autoimmune diseases occur when the immune system attacks the body's own tissues. They are more common in the elderly and in women, and may be triggered by genetic, hormonal, environmental, or infectious factors.
Estrogen may stimulate cytotoxic T cell activity.
Maternal or fetal cells crossing the placenta can trigger autoimmunity.
Environmental triggers include viral infections and molecular mimicry.
Genetic predisposition (e.g., certain MHC genes).
Failure of immune regulation mechanisms.
Examples of Autoimmune Diseases
Systemic autoimmune diseases: Affect multiple organs (e.g., SLE, rheumatoid arthritis).
Single-organ autoimmune diseases: Target specific tissues (e.g., blood cells, endocrine glands, nervous tissue).
Autoimmunity Affecting Blood Cells
Autoimmune hemolytic anemia: Antibodies against red blood cells cause severe anemia. May follow viral infection or drug treatment.
Autoimmunity Affecting Endocrine Organs
Type 1 diabetes mellitus: Immune destruction of pancreatic islets leads to insulin deficiency.
Graves' disease: Autoantibodies stimulate the thyroid, causing hyperthyroidism and goiter. Treated with antithyroid drugs, radioactive iodine, or surgery.
Autoimmunity Affecting Nervous Tissue
Multiple sclerosis (MS): Cytotoxic T cells destroy myelin sheaths, impairing neural function.
Immunodeficiency Diseases
Types of Immunodeficiency Diseases
Immunodeficiency diseases result from defective immune mechanisms and are classified as primary (congenital) or acquired.
Primary immunodeficiency: Genetic or developmental defects, manifesting in infancy or childhood.
Acquired immunodeficiency: Result from external factors such as infections (e.g., HIV/AIDS), aging, stress, or malnutrition.
Examples of Primary Immunodeficiency Diseases
Disease | Defect | Manifestation |
|---|---|---|
Chronic granulomatous disease | Ineffective phagocytes | Uncontrolled infections |
Severe combined immunodeficiency disease (SCID) | Lack of T and B cells | No resistance to infection; rapid death |
DiGeorge syndrome | Lack of T cells | Overwhelming viral infections |
Bruton-type agammaglobulinemia | Lack of B cells | Overwhelming bacterial infections |
Acquired Immunodeficiency Diseases
Caused by aging, severe stress, malnutrition, or infection (e.g., HIV/AIDS).
HIV infection leads to AIDS, characterized by low CD4 T cell counts and opportunistic infections.
Micro Matters: Meningococcal Meningitis
Meningococcal meningitis is an infection of the meninges caused by Neisseria meningitidis. Rapid antibiotic treatment is critical to prevent permanent CNS damage or death.
Additional info: The notes above include expanded academic context and explanations for clarity and completeness, as well as logical grouping of fragmented topics. All tables have been recreated in HTML format, and only directly relevant images have been included to reinforce the educational content.
