 Back
BackImmune System Disorders: Hypersensitivity, Autoimmunity, and Immunodeficiency
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Immune System Disorders
Overview
Immune system disorders arise when the immune response is either excessive, misdirected, or insufficient. These disorders include hypersensitivity reactions (allergies), autoimmune diseases, and immunodeficiency syndromes. Understanding these conditions is crucial for recognizing how the immune system can contribute to disease as well as protection.
Hypersensitivity Reactions
Definition and General Concepts
Hypersensitivity refers to an exaggerated or inappropriate immune response to an antigen, termed an allergen.
These reactions can cause tissue damage and clinical symptoms ranging from mild to life-threatening.
There are four main types of hypersensitivity reactions, classified by their mechanisms and timing.
Type I Hypersensitivity (Anaphylactic Response)
This type involves an immediate allergic reaction mediated by IgE antibodies. It is commonly associated with allergies such as hay fever, asthma, and food allergies.
First Exposure: B cells recognize the allergen and, with help from T helper cells, differentiate into plasma cells that produce IgE antibodies. These IgE molecules bind to mast cells and basophils, sensitizing them for future encounters.
Second Exposure: The allergen cross-links the IgE on mast cells or basophils, triggering the release of histamine and other mediators.
Symptoms: Vasodilation, redness, swelling, itchiness, increased mucous production, and bronchial constriction. Systemic exposure can cause anaphylactic shock, a medical emergency.


Treatments for Type I Hypersensitivity
Antihistamines: Block histamine receptors, reducing symptoms such as itching and swelling. Effective for mild allergies.
Epinephrine: Used for anaphylactic shock; acts as a vasoconstrictor to rapidly increase blood pressure and open airways.
Allergy Shots (Immunotherapy): Gradual exposure to increasing doses of allergen induces IgG production, which neutralizes the allergen before it can bind IgE, preventing histamine release.
Type II Hypersensitivity (Antibody-Dependent Cytotoxicity)
This reaction involves antibodies (IgG or IgM) directed against antigens on the surface of cells, leading to cell destruction via complement activation or phagocytosis. Commonly seen in blood transfusion reactions and hemolytic disease of the newborn.
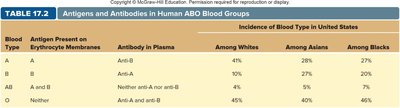
ABO Blood Group System: Antibodies target A or B antigens on red blood cells, causing agglutination and lysis if mismatched blood is transfused.
Blood Type | Antigen Present | Antibody in Plasma | Incidence Among Whites | Incidence Among Asians | Incidence Among Blacks |
|---|---|---|---|---|---|
A | A | Anti-B | 41% | 28% | 27% |
B | B | Anti-A | 10% | 27% | 20% |
AB | A and B | Neither anti-A nor anti-B | 4% | 5% | 7% |
O | Neither | Anti-A and anti-B | 45% | 40% | 46% |
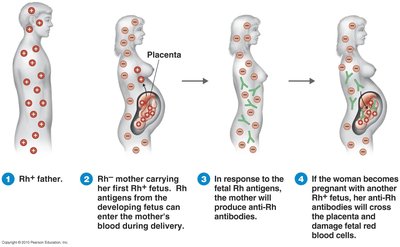
Rh Factor: An antigen on red blood cells. If an Rh- mother carries an Rh+ fetus, she may develop anti-Rh antibodies that can attack the red blood cells of subsequent Rh+ fetuses, causing hemolytic disease of the newborn.
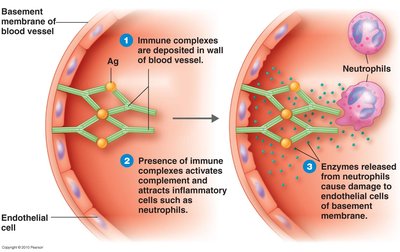
Type III Hypersensitivity (Immune Complex-Mediated)
This reaction occurs when antigen-antibody complexes form in the bloodstream and deposit in tissues, leading to inflammation and tissue damage. The complexes activate complement and attract neutrophils, which release enzymes that damage tissues.
Symptoms: Inflammation, tissue damage, especially in blood vessels, kidneys, and joints.
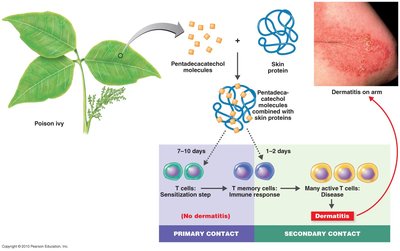
Type IV Hypersensitivity (Delayed-Type, Cell-Mediated)
This reaction is mediated by T cells, not antibodies, and typically occurs 24–72 hours after exposure to the antigen. It is responsible for contact dermatitis and some transplant rejection reactions.
Mechanism: Small chemicals bind to skin proteins, forming new antigens that activate memory T cells. Cytotoxic T cells then attack the altered skin cells, causing localized inflammation.
Example: Contact dermatitis from poison ivy exposure.

Transplantation and Graft Rejection
Immune Response to Transplants
Transplanted tissues with different MHC molecules are recognized as foreign and attacked by cytotoxic T cells (Tc) and natural killer (NK) cells.
Immunosuppressive drugs (e.g., cyclosporin) are used to prevent rejection but increase infection risk.
Graft vs Host Disease: Donor T cells attack the recipient's tissues, especially after bone marrow transplants.
Immunodeficiency Disorders
Types and Examples
Primary (Congenital) Immunodeficiency: Genetic defects resulting in non-functional T and/or B cells (e.g., Severe Combined Immunodeficiency Disease, SCID).
Acquired Immunodeficiency: Caused by infections such as HIV, which destroys T helper cells, macrophages, and dendritic cells, leading to AIDS.
Autoimmune Diseases
Mechanisms and Examples
Occur when the immune system attacks the body's own tissues, possibly triggered by infection, genetic factors, or unknown causes.
Rheumatic Fever: Antibodies against Streptococcus M protein cross-react with heart tissue, causing damage.
Rheumatoid Arthritis: IgM, IgG, and complement attack collagen in joints, causing chronic inflammation.
Lupus (Systemic Lupus Erythematosus): Antibodies against chromatin (DNA-protein complex) form immune complexes that deposit in tissues.
Multiple Sclerosis: T cells and macrophages attack the myelin sheath of neurons, leading to neurological symptoms.
