Back
BackImmune System Disorders: Immunodeficiencies, Autoimmunity, and Hypersensitivity Reactions
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Immune System Disorders
Overview
Immune system disorders encompass a range of conditions where the immune system is either underactive (immunodeficiency), overactive (hypersensitivity), or misdirected against self-tissues (autoimmunity). Understanding these disorders is crucial for recognizing their clinical manifestations, underlying mechanisms, and therapeutic approaches.
Immunodeficiencies
Types of Immunodeficiencies
Immunodeficiencies are conditions where the immune system's ability to fight infectious disease and cancer is compromised or entirely absent. They are classified as primary (genetic) or secondary (acquired).
Primary Immunodeficiency: Congenital, resulting from genetic defects that affect immune factors. Over 300 disorders are known, often lifelong and sometimes severe.
Secondary Immunodeficiency: Acquired later in life due to external factors such as infections, aging, chronic diseases, or immunosuppressive drugs. More common than primary forms.
Examples of Primary Immunodeficiencies
B cell/Antibody Deficiencies: Selective IgA/IgG deficiencies, X-linked agammaglobulinemia, hyper-IgM syndrome.
T cell Deficiencies: DiGeorge syndrome, congenital thymic dysplasia, ataxia-telangiectasia.
Combined Immunodeficiencies: Severe combined immunodeficiency (SCID), Wiskott-Aldrich syndrome, common variable immunodeficiency.
Phagocyte Defects: Chronic granulomatous disease, cyclic neutropenia, Chédiak-Higashi syndrome.
Complement Deficiencies: C2, C4, C9 deficiencies.
Therapies: Bone marrow transplants, antibody administration, cytokine therapies, and experimental treatments (e.g., gene therapy).
Examples of Secondary Immunodeficiencies
Causes: Aging, infectious agents (e.g., HIV), medical interventions (immunosuppressive drugs), systemic disorders (diabetes, malnutrition).
Drug Classes: Anticonvulsants, corticosteroids, immunosuppressants.
HIV/AIDS: HIV infects CD4+ T helper cells, leading to acquired immunodeficiency syndrome (AIDS) and increased risk of infections and cancers (e.g., Kaposi sarcoma).
Autoimmune Disorders
Mechanisms and Examples
Autoimmunity arises when the immune system loses self-tolerance and attacks healthy tissues. Over 100 autoimmune diseases are described, affecting various organs and tissues.
Systemic Autoimmune Disorders: Affect multiple tissues (e.g., systemic lupus erythematosus, rheumatoid arthritis).
Localized Autoimmune Disorders: Target specific tissues (e.g., type 1 diabetes, multiple sclerosis, Hashimoto's thyroiditis).
Risk Factors: Genetics, environmental triggers, and certain infections.
Common Autoimmune Diseases by System
Respiratory: Wegener’s granulomatosis, sarcoidosis.
Neuromuscular: Multiple sclerosis, Guillain-Barré syndrome, myasthenia gravis.
Connective Tissue: Rheumatoid arthritis, scleroderma, psoriasis.
Kidneys: IgA nephropathy, Goodpasture syndrome.
Gastrointestinal: Crohn’s disease, celiac disease.
Endocrine: Graves’ disease, Hashimoto’s disease, type 1 diabetes.
Diagnosis and Management
Symptoms: Joint/muscle pain, fatigue, rash, organ dysfunction, low-grade fever.
Diagnosis: Detection of autoantibodies, self-reactive immune cells, and other hematological tests. Rarely diagnosed with a single test.
Treatment: Immunosuppression and anti-inflammatory drugs; often leads to secondary immunodeficiency.


Autoimmunity and Infectious Agents
Disease | Implicated Infectious Agents | Features |
|---|---|---|
Type 1 diabetes | Coxsackievirus B | Immune attack on pancreatic beta cells |
Guillain-Barré syndrome | Campylobacter jejuni | Peripheral nerve damage, muscle weakness |
Rheumatic heart disease | Streptococcus pyogenes | Heart inflammation, scarring |
Multiple sclerosis | Human herpesvirus 6, Epstein-Barr virus | Myelin sheath loss, delayed nerve transmission |
Hypersensitivity Reactions
Classification and Mechanisms
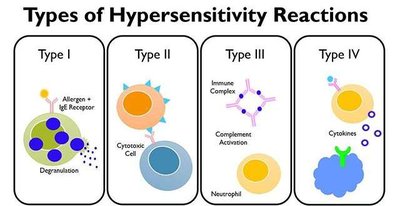
Hypersensitivities are inappropriate immune responses that can be localized or systemic. The Gell and Coombs classification divides them into four types, remembered by the mnemonic "ACID":
Type I (Allergy): IgE-mediated, rapid onset (e.g., anaphylaxis, allergic rhinitis).
Type II (Cytotoxic): IgG or IgM-mediated, targets cell surface antigens (e.g., hemolytic anemia, transfusion reactions).
Type III (Immune Complex): IgG or IgM binds soluble antigens, forming complexes that deposit in tissues (e.g., lupus, serum sickness).
Type IV (Delayed): T cell-mediated, delayed onset (e.g., contact dermatitis, transplant rejection).
Type I Hypersensitivity (Allergy)
Type I hypersensitivity involves IgE antibodies binding to allergens, leading to mast cell degranulation and release of inflammatory mediators.
Examples: Allergic rhinitis, atopic dermatitis, anaphylaxis.
Risk Factors: Family history, route of exposure, amount of IgE produced.
Diagnosis: Blood tests for IgE, skin prick tests.
Treatment: Avoidance, antihistamines, epinephrine for anaphylaxis, desensitization therapy.

Type II Hypersensitivity (Cytotoxic)
Type II reactions involve IgG or IgM antibodies binding to antigens on cell surfaces, leading to cell destruction via complement activation or antibody-dependent cellular cytotoxicity.
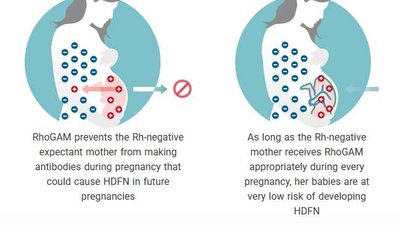
Examples: Hemolytic disease of the newborn (HDN), blood transfusion reactions, Goodpasture syndrome.
Blood Groups: A, B, AB, O, and Rh factor determine compatibility.
Prevention of HDN: Administration of RhoGAM to Rh-negative mothers.


Type III Hypersensitivity (Immune Complex)
Type III hypersensitivity is characterized by the formation of antigen-antibody complexes that deposit in tissues, activating complement and causing inflammation.
Examples: Systemic lupus erythematosus, rheumatoid arthritis, poststreptococcal glomerulonephritis.
Symptoms: Rash, joint pain, organ dysfunction depending on site of deposition.
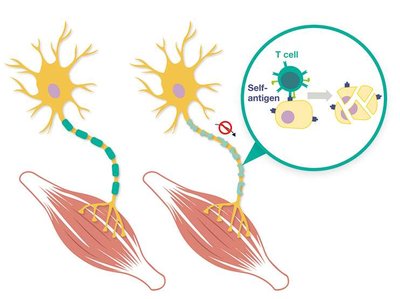
Type IV Hypersensitivity (Delayed, T Cell-Mediated)
Type IV hypersensitivity is mediated by T cells, not antibodies, and manifests 12–72 hours after antigen exposure. It is responsible for many autoimmune pathologies and contact allergies.
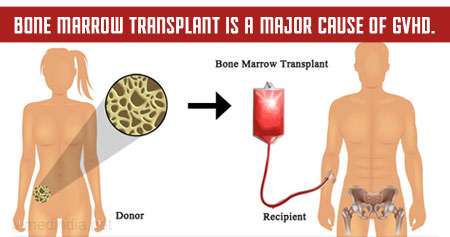
Examples: Multiple sclerosis, type 1 diabetes, Hashimoto thyroiditis, celiac disease, contact dermatitis (e.g., poison ivy), transplant rejection, graft-versus-host disease (GVHD).
Treatment: Immunosuppressive drugs, corticosteroids, cytokine blockers.

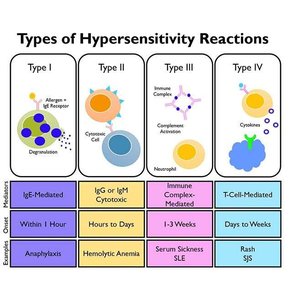
Summary Table: Hypersensitivity Types
Type | Mechanism | Onset | Examples |
|---|---|---|---|
I (Allergy) | IgE-mediated, mast cell degranulation | Minutes to 1 hour | Anaphylaxis, allergic rhinitis |
II (Cytotoxic) | IgG/IgM to cell surface antigens, complement activation | Hours to days | Hemolytic anemia, transfusion reactions |
III (Immune Complex) | IgG/IgM to soluble antigens, immune complex deposition | 1–3 weeks | Lupus, serum sickness |
IV (Delayed) | T cell-mediated | Days to weeks | Contact dermatitis, multiple sclerosis |