 Back
BackLyme Disease: Microbiology, Pathogenesis, Diagnosis, and Prevention
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Microbial Infections – Lyme Disease
Overview and History
Lyme disease is a significant vector-borne bacterial infection with acute and chronic phases, primarily affecting humans in North America and Europe. It was first identified in Lyme County, Connecticut, in 1977, when a cluster of children was initially misdiagnosed with juvenile arthritis. The disease is now recognized as a major public health concern due to its prevalence and potential for chronic complications.
Causative Agent
Borrelia burgdorferi: The primary causative agent, a Gram-negative spirochete bacterium.
Borrelia mayonii: A rare, related Gram-negative spirochete.
Taxonomy Note: The genus Borrelia may also be referred to as Borreliella in some literature, though this change is not yet widely adopted in clinical practice.

Transmission and Life Cycle
Reservoirs: Small mammals and birds serve as natural reservoirs for Borrelia species.
Vector: The black-legged tick (Ixodes scapularis) transmits the bacteria to humans. Ticks must be attached for 36–48 hours for effective transmission.
Human Infection: Most human cases occur in spring and summer, coinciding with tick activity.
Prevention Strategies
Prevention focuses on minimizing tick exposure and prompt removal of ticks. Environmental management and personal protection are key strategies.
Use of insect repellents
Prompt and proper removal of ticks
Pesticide application in tick-prone areas
Reduction of tick habitat (e.g., landscaping, removing leaf litter)

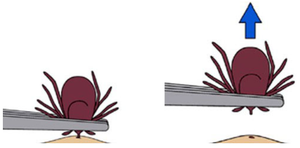
Tick Removal
Proper tick removal is essential to reduce the risk of disease transmission. Ticks should be grasped with fine-tipped tweezers as close to the skin as possible and pulled upward with steady, even pressure. Do not twist or jerk the tick. Dispose of the tick by placing it in alcohol, a sealed bag, or flushing it down the toilet. Do not crush ticks with bare fingers.
Clinical Manifestations
Early Localized Disease
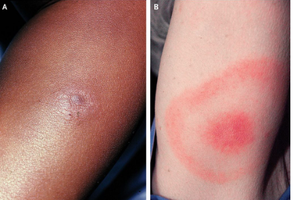
Erythema migrans (EM) rash: Occurs in 70–80% of infected individuals, typically 3–30 days after the tick bite (average 7 days). The rash gradually expands and may reach 12 inches or more, often with a characteristic "bull's-eye" appearance (annular lesion).
Note: EM may be less visible or atypical in patients with darker skin tones, leading to underdiagnosis.
Early Disseminated Disease
Secondary EM lesions across the body
Systemic symptoms: headache, neck stiffness, fever, chills, arthralgias, muscle aches, profound malaise
Neurologic involvement: meningitis, encephalitis, cranial neuritis, neuropathy, ataxia, myelitis
Cardiac complications (rare): atrioventricular block, myopericarditis, cardiomegaly
Late Disease
Arthritis, especially in large joints (e.g., knee), lasting weeks to months
Chronic neurological issues: encephalopathy affecting mood, memory, and sleep (may persist for years)
Rash Variability
The appearance of Lyme disease rashes can vary widely in color, shape, and location, making clinical recognition challenging.

Diagnosis
Assessment of clinical signs and symptoms
Evaluation of possible tick exposure
Consideration of differential diagnoses (other diseases with similar presentations)
Laboratory Testing
ELISA (Enzyme-Linked Immunosorbent Assay): Initial screening test for antibodies against B. burgdorferi. A negative result rules out Lyme disease, but a positive result only indicates exposure, not necessarily active infection. Early negative results may not be informative due to delayed antibody production.

Western Blot: Confirmatory test for IgM and IgG antibodies. Interpretation depends on the number of specific antibody bands detected:
IgM: 2 of 3 bands positive within the first 4 weeks
IgG: 5 of 10 bands positive after 4 weeks
Treatment
Early localized/disseminated disease: Doxycycline (100 mg twice daily), amoxicillin (500 mg three times daily), or cefuroxime axetil (500 mg twice daily) for 14 days.
Neurologic involvement: Ceftriaxone (2 g IV daily) for 14 days.
Cardiac manifestations: Oral or parenteral antibiotics for 14 days.
Vaccine Development
Recent vaccine candidates (e.g., Pfizer) target the six most common B. burgdorferi outer surface protein A types.
Phase 3 trials showed 70–73% efficacy, but the vaccine did not meet all endpoints for approval.
Incidence and Surveillance
Estimated 476,000 cases annually (insurance claims data); CDC estimates 300,000 cases per year.
Only about 35,000 cases are reported annually due to passive surveillance and underreporting.
Special Considerations
Other tick-borne diseases: babesiosis, Rocky Mountain spotted fever, Powassan virus, anaplasmosis/ehrlichiosis
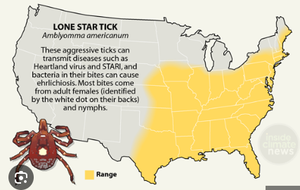
Alpha-gal syndrome: An emerging allergic condition to red meat or gelatin-coated medications, associated with the bite of the lone star tick (Amblyomma americanum).
Additional info: Lyme disease is a model for understanding vector-borne zoonoses, the importance of early diagnosis, and the challenges of vaccine development for complex bacterial pathogens.
