 Back
BackMicrobe–Human Interactions: Infection, Disease, and Epidemiology
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Microbe–Human Interactions
Overview of Microbial Relationships with Humans
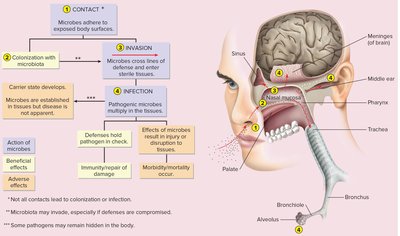
The human body is host to approximately 100 trillion microbes, forming a dynamic equilibrium with microorganisms. This balanced coexistence is essential for health, as microbes provide protective effects, aid in immune system maturation, and can cause disease if they invade sterile tissues.
Protective Effects: Microbes establish themselves as normal residents, stabilizing body surfaces.
Immune System Development: Microbes contribute to the maturation of host defenses.
Pathogenic Potential: Microbes may invade sterile tissues, causing disease by damaging organs.

Microbe Relationship with Human Body
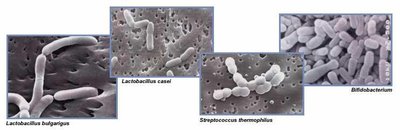
Microbes that engage in mutual or commensal associations with humans are termed normal resident microbiota or indigenous microflora. These are restricted to outer surfaces and do not penetrate sterile tissues or fluids. When microbes breach host defenses and invade sterile tissue, they become infectious agents and may cause disease.
Resident Microbiota: The Human as Habitat
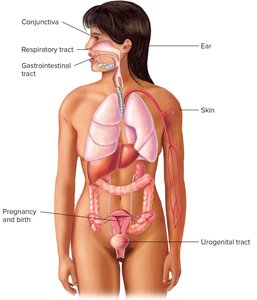
Sites Harboring Normal Resident Microbes
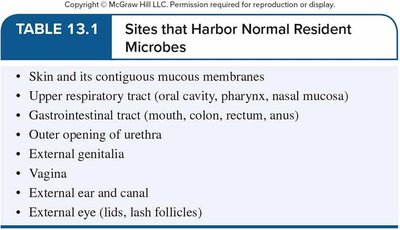
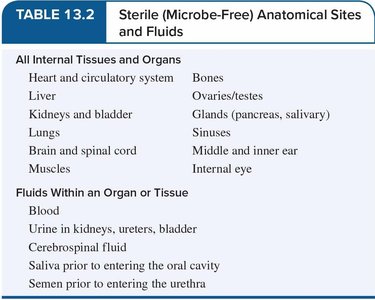
Resident microbiota occupy a wide range of habitats, including areas with variations in temperature, pH, nutrients, moisture, and oxygen tension. Most areas in contact with the external environment harbor resident microbes, while internal organs, tissues, and fluids are microbe-free.
Sites that Harbor Normal Resident Microbes |
|---|
Skin and its contiguous mucous membranes |
Upper respiratory tract (oral cavity, pharynx, nasal mucosa) |
Gastrointestinal tract (mouth, colon, rectum, anus) |
Outer opening of urethra |
External genitalia |
Vagina |
External ear and canal |
External eye (lids, lash follicles) |
Sterile (Microbe-Free) Anatomical Sites and Fluids |
|---|
All Internal Tissues and Organs: Heart, liver, kidneys, lungs, brain, muscles, bones, ovaries/testes, glands, sinuses, middle/inner ear, internal eye |
Fluids Within an Organ or Tissue: Blood, urine (in kidneys, ureters, bladder), cerebrospinal fluid, saliva (prior to entering oral cavity), semen (prior to entering urethra) |
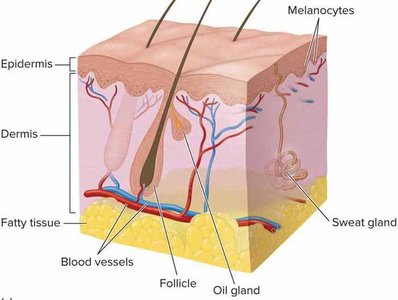
Types of Cutaneous Populations
Microbiota reside only on dead cell layers of the skin. Transition zones (nose, mouth, external genitalia) are rich in microbes. There are two types of cutaneous populations:
Transients: Cling to the surface but do not grow; influenced by hygiene.
Residents: Stable, predictable, less affected by hygiene; include bacteria and yeasts.
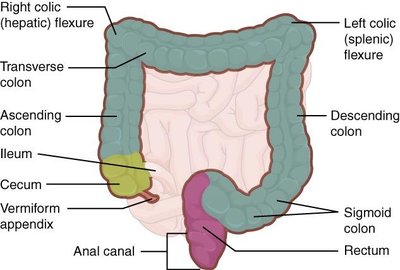
Microbiota of the Gastrointestinal Tract
Distribution and Function
The GI tract is a long hollow tube exposed to the environment, with flora distribution varying due to shifting conditions (pH, oxygen tension, anatomy). The mouth harbors the most diverse microflora, while the large intestine and rectum contain large populations of microbes, predominantly strict anaerobes.
Fermentation: Produces vitamins (B12, K, pyridoxine, riboflavin, thiamine) and acids (acetic, butyric, propionic).
Enzymatic Activity: Aids in carbohydrate digestion and steroid metabolism.
Odor Production: Intestinal bacteria contribute to intestinal odor (skatole).
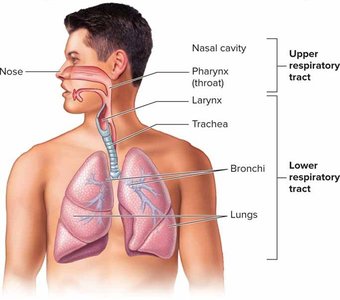
Microbiota of the Respiratory Tract
Colonization and Defense
The upper respiratory tract (nasal passages, throat, pharynx) harbors a microbial population similar to the oral cavity. The trachea may have a sparse population, while bronchi, bronchioles, and alveoli are essentially sterile due to local host defenses.
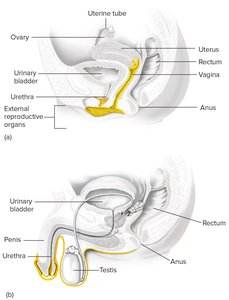
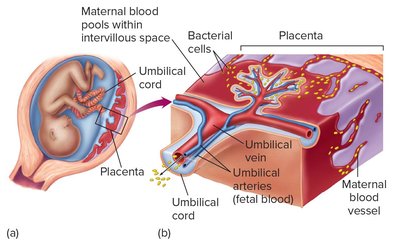
Microbiota of the Genitourinary Tract
Sites and Influences
Microflora are found in the vagina and outer opening of the urethra in females, and the anterior urethra in males. Internal reproductive organs are kept sterile through physical barriers. Changes in physiology, such as hormonal fluctuations, influence the composition of normal flora.
Maintenance and Importance of Normal Microbiota
Health Implications
Normal flora is essential to human health, creating an environment that prevents infections and enhances host defenses. Antibiotics, dietary changes, and disease may alter flora. Probiotics are used to reintroduce beneficial microbes.

Chain of Infection and Pathogenicity
Pathogen Types and Virulence
Pathogens are classified based on their ability to cause disease:
True Pathogens: Cause disease in healthy individuals (e.g., Influenza virus).
Opportunistic Pathogens: Cause disease when host defenses are compromised (e.g., Pseudomonas sp., Candida albicans).
Virulence Factors: Characteristics or structures that contribute to a microbe's ability to cause disease.

Portals of Entry and Infectious Dose
Routes of Entry
Microbes enter the body via characteristic routes known as portals of entry, which include the skin, GI tract, respiratory tract, and urogenital tract. The source may be exogenous (outside the body) or endogenous (from microbiota or latent infection).
Infectious Dose (ID)
The minimum number of microbial cells or particles required to initiate infection is termed the infectious dose (ID). This varies by pathogen and route of infection.
Virulence Factors and Host Interaction
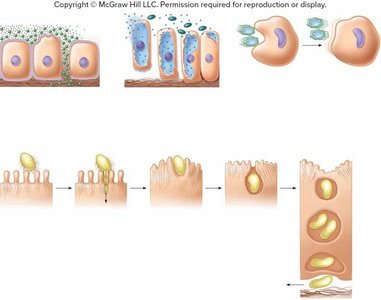
Attachment and Invasion
Pathogens must attach firmly to host cells to establish infection. This is achieved through appendages and surface structures (flagella, fimbriae, pili, adhesive slimes, capsules), viral spikes, or hooks and suckers in parasites.
Immune Evasion and Tissue Invasion
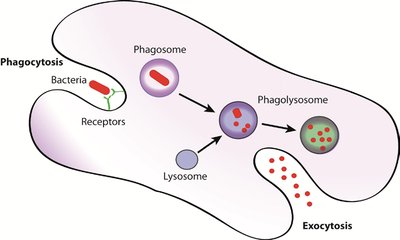
Virulence factors include mechanisms to evade host defenses, such as antiphagocytic factors (capsules, leukocidins), production of extracellular enzymes (exoenzymes), and toxins.
Exoenzymes: Dissolve barriers and promote spread in deeper tissues.
Toxins: Damage target cells, causing disease symptoms.
Antiphagocytic Factors: Prevent engulfment by phagocytes.




Key Exoenzymes and Their Effects
Microbe | Enzyme | Function/Effect |
|---|---|---|
Streptococcus pyogenes | Hyaluronidase | Breaks down connective tissue, spreads infection |
Clostridium perfringens | Collagenase | Degrades collagen, facilitates tissue invasion |
Staphylococcus aureus | Coagulase | Forms blood clots, shields bacteria |
Escherichia coli | Urease | Increases urine pH, aids urinary tract infection |
Treponema pallidum | Hyaluronidase | Spreads through skin and mucous membranes |
Mycobacterium tuberculosis | Phospholipase C | Facilitates escape from host cell vacuoles |
Helicobacter pylori | Mucinase | Breaks down gastric mucins, penetrates stomach lining |
Bacterial Toxins
Bacterial toxins are specific chemical products that have poisonous effects on other organisms. They are classified as exotoxins (secreted by living cells) and endotoxins (released after cell damage).


Characteristic | Exotoxins | Endotoxin |
|---|---|---|
Toxicity | Toxic in small amounts | Toxic in higher quantities |
Effects on Body | Specific to cell type | Systemic, less specific |
Chemical Composition | Small proteins | Lipopolysaccharide |
Heat Denaturation | Unstable | Stable |
Toxoid Formation | Can be converted | Cannot be converted |
Immune Response | Stimulate antitoxins | No antitoxins |
Fever Stimulation | Usually not | Yes |
Manner of Release | Secreted from live cell | Released during lysis |
Typical Sources | Gram-positive and gram-negative | All gram-negative |
Examples | Tetanus, diphtheria, cholera | Meningitis, endotoxic shock |
The Process of Infection and Disease
Stages of Clinical Infection
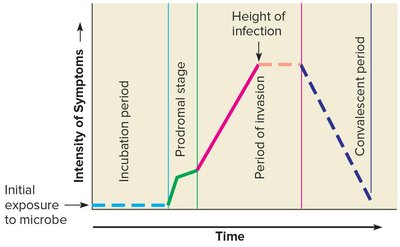
Clinical infections progress through four distinct stages:
Incubation Period: Time from initial contact to first symptoms; agent multiplies but damage is insufficient for symptoms.
Prodromal Stage: Initial vague symptoms; lasts 1-2 days.
Period of Invasion: Pathogen multiplies at high levels; specific signs and symptoms appear.
Convalescent Period: Symptoms decline as immune system clears the agent; recovery occurs.
Patterns of Infection
Types and Sequence
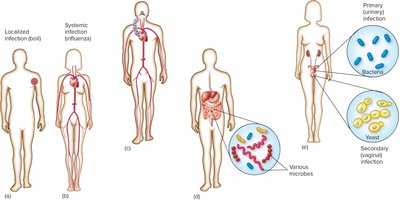
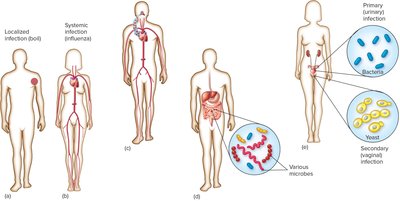
Localized Infection: Confined to a specific tissue (e.g., boils, warts).
Systemic Infection: Spreads to several sites, often via bloodstream.
Focal Infection: Agent breaks loose from local infection and spreads.
Toxemia: Toxins produced locally are carried by blood to target tissues.
Mixed Infection: Several microbes grow simultaneously at the site.
Primary Infection: Initial infection.
Secondary Infection: Complication by another microbe.
Acute Infection: Rapid onset, severe, short-lived.
Chronic Infection: Progresses and persists over long period.
Signs and Symptoms of Disease
Definitions and Examples
Sign: Objective evidence of disease (e.g., fever, rash, high blood pressure).
Symptom: Subjective evidence sensed by the patient (e.g., pain, fatigue, nausea).
Syndrome: Disease identified by a collection of signs and symptoms.
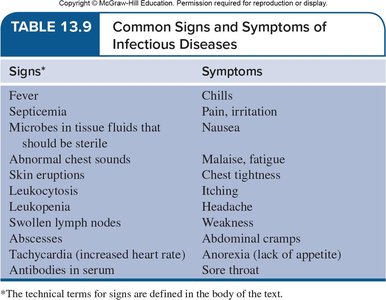
Signs | Symptoms |
|---|---|
Fever | Chills |
Septicemia | Pain, irritation |
Microbes in sterile fluids | Nausea |
Abnormal chest sounds | Malaise, fatigue |
Skin eruptions | Chest tightness |
Leukocytosis | Itching |
Leukopenia | Headache |
Swollen lymph nodes | Weakness |
Abscesses | Abdominal cramps |
Tachycardia | Anorexia |
Antibodies in serum | Sore throat |
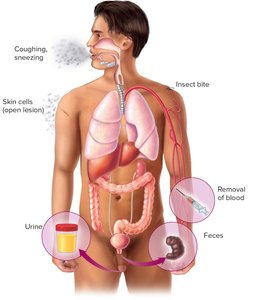
Portals of Exit and Persistence
Pathogen Departure and Latency
Pathogens depart the host via specific avenues, influencing dissemination. Recovery does not always mean the microbe is removed; some may persist in a latent state or as chronic carriers.
Epidemiology
Origins, Transmission, and Reservoirs
Epidemiology is the study of disease frequency and distribution in populations. Pathogens may have living (human, animal) or non-living (soil, water) reservoirs. Transmission can be direct or indirect, and diseases may be communicable or non-communicable.


Patterns of Disease Occurrence
Endemic: Steady frequency in a geographic locale.
Sporadic: Occasional cases at irregular intervals.
Epidemic: Prevalence increases beyond expected.
Pandemic: Epidemic across continents.
Nosocomial Infections
Nosocomial (health-care-associated) infections are acquired during hospital stays, often involving surgical sites, respiratory tract, GI tract, skin, urinary tract, and blood. Prevention includes isolation precautions and universal blood and body fluid precautions.
Patterns of Disease: Disease Cycle
Summary of Disease Process
Survival outside host (reservoir)
Transmission to host
Portal of entry
Attachment to target tissue
Colonization
Host damage
Portal of exit
Virulence Measurement
Virulence can be measured experimentally by determining the lethal dose 50 (LD50) or infectious dose 50 (ID50):
ID50: Dose infecting 50% of hosts.
LD50: Dose killing 50% of hosts.
Summary Table: Exotoxin vs. Endotoxin
Characteristic | Exotoxin | Endotoxin |
|---|---|---|
Source | Mainly Gram +ve | Gram –ve only |
Metabolic product | By-products of growing cell | Part of cell wall |
Chemistry | Protein | Lipid |
Fever? | No | Yes |
Neutralized by antitoxin | Yes | No |
LD50 | Small | Relatively large |
Additional info: These notes expand on the original content by providing definitions, examples, and structured tables for clarity. All included images directly reinforce the adjacent educational content.
