Back
BackMicrobial Diseases of the Digestive System: Structure, Function, and Pathogenesis
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Digestive System Overview
Structure and Function of the Digestive System
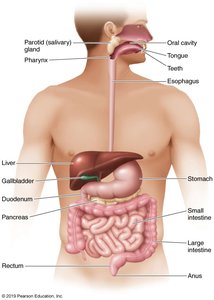
The digestive system, also known as the gastrointestinal (GI) tract or alimentary canal, is responsible for the breakdown and absorption of nutrients, as well as immune defense. It consists of the mouth, pharynx, esophagus, stomach, small and large intestines, and accessory organs such as the teeth, tongue, salivary glands, liver, gallbladder, and pancreas.
Preparation of Food: Mechanical and chemical processes prepare food for absorption.
Absorption of Nutrients: Most nutrients are absorbed in the small intestine.
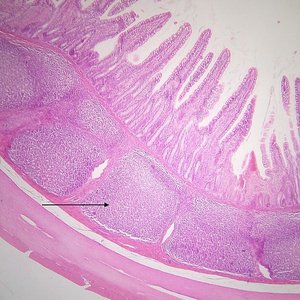
Immune Function: Approximately 80% of immune system structures are located in the intestinal tract, including gut-associated lymphoid tissue (GALT), lymph nodes, and Peyer’s patches.
Histology and Immune Structures
Peyer’s patches are lymphoid follicles found in the small intestine, playing a crucial role in immune surveillance and response to pathogens entering through the gut.
Normal Microbiota of the Digestive System
Distribution and Function
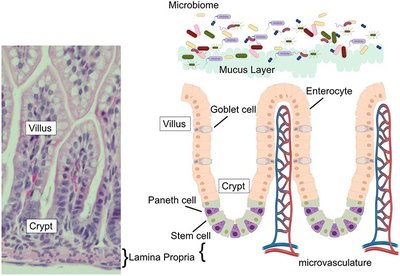
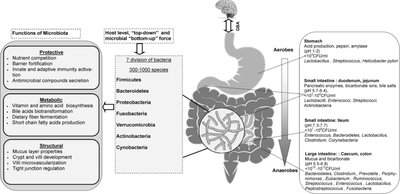
The digestive tract harbors a diverse microbiota, with the highest density in the large intestine. The composition and function of these microbes are essential for health, digestion, and immune modulation.
Mouth: Millions of bacteria per milliliter of saliva.
Stomach: Few microorganisms due to low pH and hydrochloric acid (HCl) production.
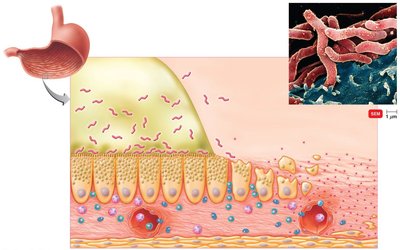
Small Intestine: Paneth cells produce antimicrobial proteins (defensins) and phagocytose microbes.
Large Intestine: Contains large numbers of anaerobes and facultative anaerobes; up to 100 billion bacteria per gram of feces.
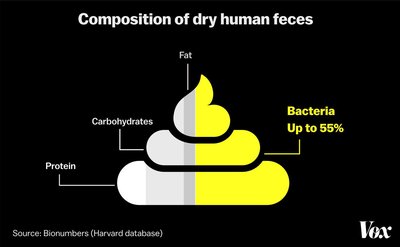
Microbial Contribution to Feces
Bacteria can constitute up to 55% of the dry weight of human feces, highlighting the significant microbial presence in the large intestine.
Bacterial Infections of the Digestive System
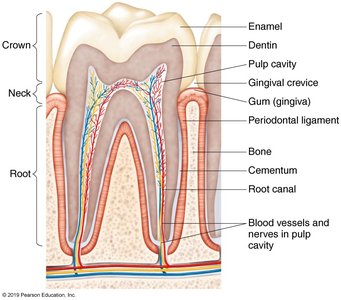
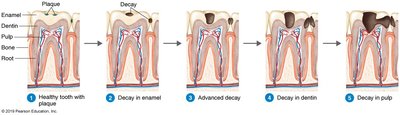
Dental Caries (Tooth Decay)
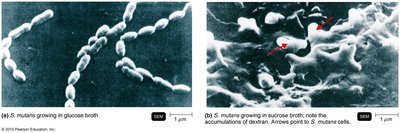
Dental caries are caused by the demineralization of tooth enamel and dentin due to acid production by bacteria, primarily Streptococcus mutans. This organism metabolizes sucrose to lactic acid and produces dextran, a polysaccharide that forms dental plaque and biofilms.
Progression: Caries penetrate from enamel into dentin and may reach the pulp, leading to abscesses.
Risk Factors: High sugar intake increases caries risk; before antibiotics, mortality from dental abscesses was significant.
Systemic Effects: Oral bacteria may contribute to heart disease and systemic inflammation.
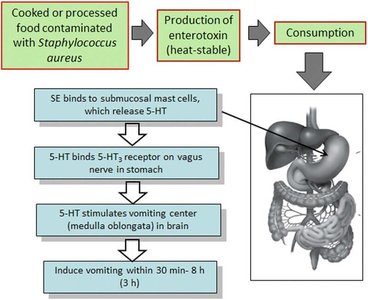
Staphylococcal Food Poisoning
Staphylococcal food poisoning is caused by ingestion of enterotoxins produced by Staphylococcus aureus in contaminated food. The toxin is heat-stable and not destroyed by boiling.
Pathogenesis: Toxin binds to receptors in the gut, stimulating the vomiting center in the brain and causing rapid onset vomiting.
Prevention: Proper food handling and storage are essential to prevent toxin production.
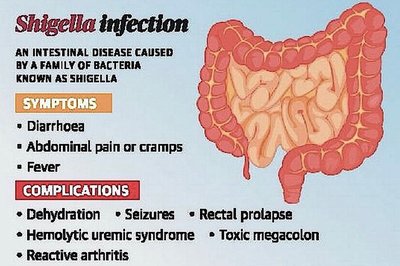
Shigellosis (Bacillary Dysentery)
Shigellosis is caused by Shigella species, which are Gram-negative, facultatively anaerobic rods. The bacteria produce Shiga toxin, invade M cells in the intestinal epithelium, and cause tissue damage and dysentery.
Symptoms: Diarrhea, abdominal pain, fever.
Complications: Dehydration, seizures, hemolytic uremic syndrome, and more.
Treatment: Fluoroquinolones and oral rehydration.

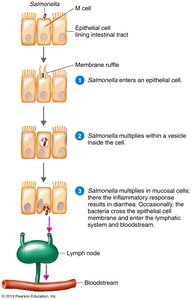
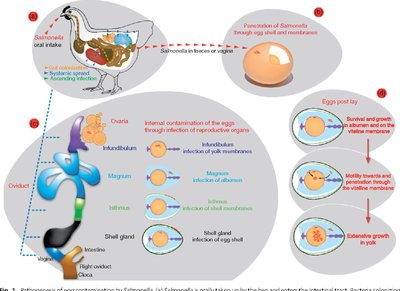
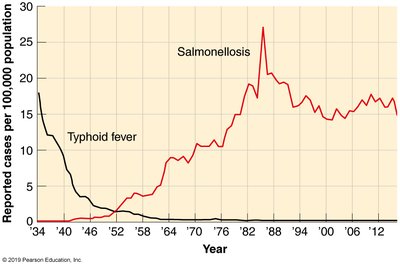
Salmonellosis (Salmonella Gastroenteritis)
Salmonellosis is caused by Salmonella enterica, a Gram-negative, facultative anaerobe. It is a common cause of foodborne illness, often associated with poultry and eggs.
Pathogenesis: Bacteria invade intestinal mucosa, replicate in macrophages, and may enter the bloodstream.
Symptoms: Fever, nausea, abdominal pain, diarrhea.
Diagnosis: Stool sample culture, PCR.
Treatment: Oral rehydration therapy.

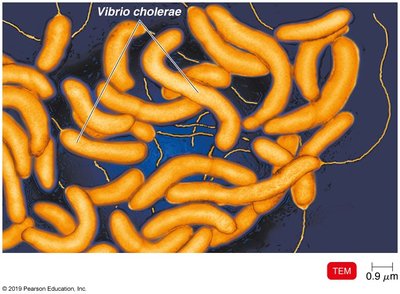
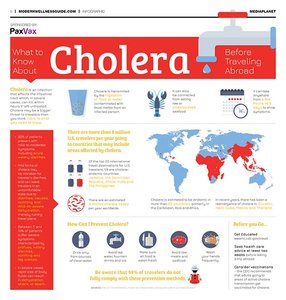
Cholera
Cholera is caused by Vibrio cholerae, a Gram-negative, curved rod with a single polar flagellum. The bacterium produces cholera toxin, which induces massive secretion of electrolytes and water, resulting in severe watery diarrhea ("rice water stools").
Transmission: Contaminated water, especially after natural disasters.
Symptoms: Rapid fluid loss, shock, organ failure.
Treatment: Immediate IV fluid replacement is critical.
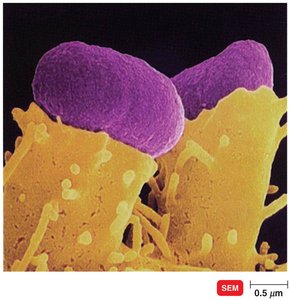
E. coli Gastroenteritis
Escherichia coli causes several types of gastroenteritis, with different pathotypes responsible for varying clinical presentations:
Enteropathogenic E. coli (EPEC): Causes diarrhea in developing countries; bacteria attach to host cells forming pedestals.
Enteroinvasive E. coli (EIEC): Causes Shigella-like dysentery.
Enteroaggregative E. coli (EAEC): Produces enterotoxin causing watery diarrhea.
Enterohemorrhagic E. coli (EHEC): Produces Shiga-like toxin, causes hemorrhagic colitis and hemolytic uremic syndrome; O157:H7 is the most common serotype.
Traveler’s Diarrhea
Traveler’s diarrhea is most commonly caused by E. coli, but can also be due to Salmonella, Shigella, or Campylobacter. It is typically self-limiting and treated with oral rehydration and bismuth preparations.

Other Notable Bacterial Infections
Clostridium difficile-Associated Diarrhea
Clostridium difficile is a Gram-positive, endospore-forming anaerobe that causes life-threatening colitis, especially after prolonged antibiotic use. It is a major cause of healthcare-associated infections and can lead to ulceration and perforation of the intestinal wall.
Peptic Ulcer Disease
Peptic ulcers are primarily caused by Helicobacter pylori, which survives stomach acid by producing urease, converting urea to ammonia and neutralizing gastric acid. The bacterium disrupts the mucosal layer, causing inflammation and ulceration.
Diagnosis: Biopsy, culture, urea breath test.
Treatment: Antimicrobial drugs and bismuth subsalicylate.