 Back
BackMicrobial Diseases of the Nervous System and Eye: Structure, Pathogenesis, and Clinical Aspects
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Structure of the Nervous System
Overview of Nervous System Organization
The nervous system is divided into two main parts: the Central Nervous System (CNS) and the Peripheral Nervous System (PNS). The CNS consists of the brain and spinal cord, while the PNS includes all neural elements outside the CNS, such as cranial and spinal nerves. These systems coordinate voluntary and involuntary actions and transmit signals throughout the body.
CNS: Brain (cerebrum, cerebellum, brain stem) and spinal cord
PNS: Cranial nerves, spinal nerves, sensory and motor pathways
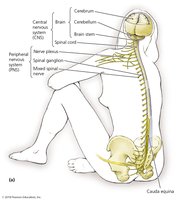
Structures of the Central Nervous System
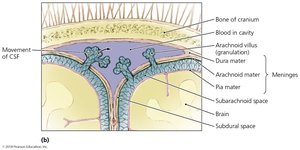
The CNS is protected by the cranium, vertebral column, and three layers of meninges (dura mater, arachnoid mater, pia mater). The subarachnoid space contains cerebrospinal fluid (CSF), which cushions the CNS, provides nutrients, and removes waste. The blood-brain barrier restricts passage of most microbes and large molecules from the blood into the CSF, maintaining the CNS as an axenic (microbe-free) environment.
Cerebrum: Controls voluntary muscles, perception, and cognition
Cerebellum: Coordinates involuntary movements
Brain stem: Regulates vital functions (breathing, heart rate, blood pressure)
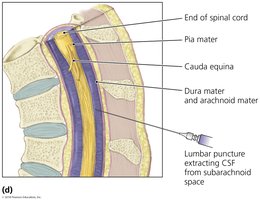
Spinal cord: Transmits signals between brain and body; ends at lumbar region, below which is the cauda equina (nerve bundle)
CSF Collection and Clinical Relevance
Medical providers collect CSF from the lower back (lumbar region) because the spinal cord does not extend into this area, reducing the risk of CNS injury or infection. The lumbar vertebrae are large and easily accessible, making lumbar puncture safer.
Structures of the Peripheral Nervous System
The PNS transmits commands from the CNS to muscles and glands and relays sensory information to the CNS. It includes cranial nerves (from the brain) and spinal nerves (from the spinal cord). Nerves are classified as sensory (to CNS), motor (from CNS), or mixed (both directions).
Cells of the Nervous System
The nervous system contains two main cell types: neuroglia (support, insulate, and nourish neurons; phagocytize microbes) and neurons (transmit nerve impulses). Neurons have a cell body (with nucleus), dendrites (receive signals), and axons (send signals). Collections of neuron cell bodies are called ganglia.
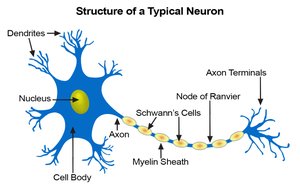
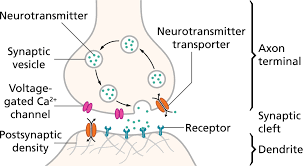
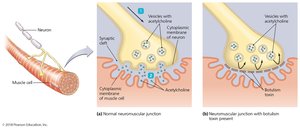
Synapses
Synapses are junctions between axons and other cells (neurons, muscles, glands). Neurotransmitters released into the synaptic cleft can stimulate or inhibit the next cell, allowing for complex signaling.
Portals of Infection of the Central Nervous System
Mechanisms of Microbial Entry
The CNS is normally sterile, but pathogens can enter through:
Breaks in bones or meninges (trauma, surgery)
Medical procedures
Travel along peripheral nerves
Crossing the blood-brain barrier (especially during inflammation)
Microbes in the blood or lymph can infect the meninges, causing meningitis.
Bacterial Diseases of the Nervous System
General Mechanisms
Bacteria cause nervous system disease by directly infecting neural tissue (e.g., meningitis, leprosy) or by releasing toxins that affect neurons (e.g., botulism, tetanus).
Bacterial Meningitis
Bacterial meningitis is an acute inflammation of the meninges, often rapidly fatal without treatment. Symptoms include fever, headache, stiff neck, nausea, vomiting, confusion, and sometimes petechiae (skin hemorrhages). Diagnosis is by CSF analysis (increased white blood cells, turbid appearance) and culture.
Five main causative agents: Neisseria meningitidis, Streptococcus pneumoniae, Haemophilus influenzae, Listeria monocytogenes, Streptococcus agalactiae
All possess virulence factors to evade phagocytosis
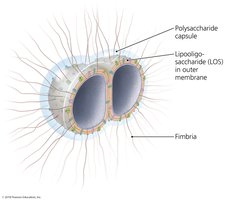
Neisseria meningitidis
Gram-negative cocci (meningococcus)
Virulence factors: fimbriae, polysaccharide capsule, lipooligosaccharide (LOS) with Lipid A endotoxin
Capsule allows survival in phagocytes; LOS triggers inflammation, shock, and clotting
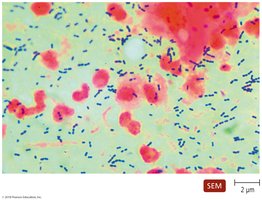
Streptococcus pneumoniae
Gram-positive coccus, often in pairs
Capsule prevents phagocytosis; phosphorylcholine triggers endocytosis, allowing invasion of blood and brain
Leading cause in children <5 and elderly
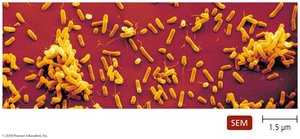
Haemophilus influenzae
Pleomorphic bacillus, obligate parasite
Capsule resists phagocytosis; type b was most common before vaccine
Listeria monocytogenes
Gram-positive coccobacillus, foodborne
Virulence: survives phagocytosis by escaping phagosome, grows in cytosol
Risk: pregnant women, newborns, elderly, immunocompromised
Streptococcus agalactiae
Group B streptococcus, normal vaginal microbiota in ~1/3 women
Capsule prevents phagocytosis
Leading cause of neonatal meningitis
Diagnosis, Treatment, and Prevention of Bacterial Meningitis
Diagnosis: symptoms, CSF analysis, culture
Treatment: intravenous antimicrobials
Prevention: vaccines (S. pneumoniae, H. influenzae type b, N. meningitidis), prophylactic antibiotics for at-risk newborns, avoiding high-risk foods for listeriosis
Hansen’s Disease (Leprosy)
Caused by Mycobacterium leprae. Two forms:
Tuberculoid leprosy: Strong T cell response, localized nerve damage, loss of sensation
Lepromatous leprosy: Weak T cell response, widespread tissue destruction, deformities
Mycolic acid in cell wall confers slow growth, resistance to phagocytosis and drugs. Transmission is by prolonged contact; not highly contagious. Diagnosis by acid-fast staining; treatment is prolonged multidrug therapy. BCG vaccine offers some protection.

Botulism
Botulism is usually an intoxication by botulinum toxin from Clostridium botulinum. Toxin blocks acetylcholine release at neuromuscular junctions, causing flaccid paralysis. Three forms: foodborne, infant (intestinal colonization), and wound botulism. Diagnosis is clinical; treatment includes airway management, antitoxin, and supportive care. Prevention: proper food handling, no honey for infants.
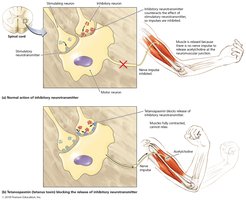
Tetanus
Caused by Clostridium tetani neurotoxin (tetanospasmin), which blocks inhibitory neurotransmitter release, resulting in spastic paralysis (lockjaw, muscle rigidity). Acquired through wounds contaminated with endospores. Diagnosis is clinical; treatment includes wound care, antitoxin, antimicrobials, and vaccination. Prevention: DTaP/Tdap vaccine.

Viral Diseases of the Nervous System
Viral Meningitis
Most common form of meningitis, usually milder than bacterial. Caused mainly by enteroviruses (coxsackie A, B, echovirus). Transmission is fecal-oral; diagnosis by exclusion of bacteria in CSF. Treatment is supportive.
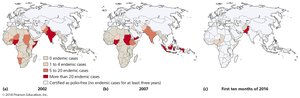
Poliomyelitis
Caused by poliovirus, transmitted via contaminated water. Most infections are asymptomatic; some cause paralysis. Vaccines have nearly eradicated polio worldwide.
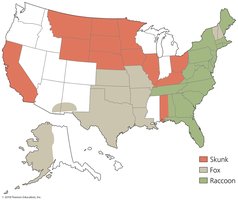
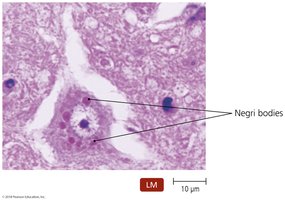
Rabies
Caused by rabies virus, transmitted by animal bites (zoonosis). Virus travels from muscle to CNS, causing neurological symptoms (hydrophobia, seizures, paralysis). Diagnosis by symptoms, antibody tests, and Negri bodies in brain tissue. Treatment: post-exposure prophylaxis (immunoglobulin, vaccine). Prevention: animal vaccination.
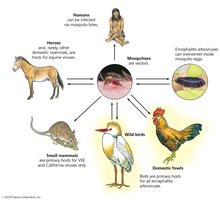
Arboviral Encephalitis
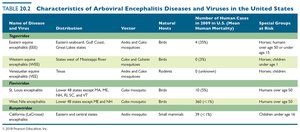
Caused by arthropod-borne viruses (e.g., West Nile virus, EEE, WEE, VEE, SLE, California encephalitis). Transmitted by mosquitoes; humans and horses are dead-end hosts. Symptoms range from mild to severe encephalitis. Diagnosis by serology; treatment is supportive. Prevention: mosquito control, vaccines for horses.
Name of Disease and Virus | Distribution | Vector | Natural Hosts | Number of Human Cases (Mean Mortality) | Special Groups at Risk |
|---|---|---|---|---|---|
Eastern equine encephalitis | Eastern Gulf Coast, Great Lakes states | Aedes and Culex mosquitoes | Birds | 6 (50%) | Humans, horses, children under age 15 |
Western equine encephalitis | Western U.S., Canada | Culex mosquitoes | Birds | 0 (3%) | Humans, horses, children under age 15 |
Venezuelan equine encephalitis | South America, Mexico, Texas, FL | Aedes and Culex mosquitoes | Rodents | 0 (1%) | Humans, horses, children under age 15 |
St. Louis encephalitis | Lower 48 states except MA, NE, NH, RI, and VT | Culex mosquitoes | Birds | 80 (5-30%) | Humans, elderly |
West Nile encephalitis | Eastern and central states | Aedes mosquitoes | Small mammals | 39 (7%) | Children under age 16 |
California encephalitis | Eastern and central states | Aedes mosquitoes | Small mammals | 39 (7%) | Children under age 16 |
Mycoses of the Nervous System
Cryptococcal Meningitis
Caused by Cryptococcus neoformans, a yeast found in soil and bird feces. Infection begins in the lungs and may spread to the CNS, especially in immunocompromised patients (e.g., AIDS). Capsule resists phagocytosis. Diagnosis: fungal antigen in CSF; treatment: intravenous antifungals.
Protozoan Diseases of the Nervous System
African Sleeping Sickness (African trypanosomiasis)
Caused by Trypanosoma brucei, transmitted by tsetse flies. Disease progresses from local lesion to blood/lymph involvement, then CNS invasion (meningoencephalitis, coma, death). Characterized by waves of parasitemia due to antigenic variation. Diagnosis: microscopy; treatment: stage-dependent drugs; prevention: vector control.

Primary Amebic Meningoencephalopathy
Caused by Acanthamoeba and Naegleria, free-living amoebae in warm water and soil. Infection is rare but usually fatal, entering through skin, eyes, or inhalation. Diagnosis: microscopy; treatment: limited success; prevention: avoid contaminated water.
Prion Diseases
Variant Creutzfeldt-Jakob Disease (vCJD)
Caused by abnormal prion proteins, leading to spongiform encephalopathies (brain tissue with holes). Symptoms: insomnia, memory loss, muscle control loss. Transmission: eating contaminated meat, medical procedures. Diagnosis: clinical, lab tests; no treatment; prevention: avoid prion-contaminated meat.
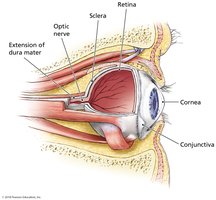
Microbial Diseases of the Eye
Trachoma
Leading cause of nontraumatic blindness, caused by Chlamydia trachomatis. Infection scars conjunctiva and cornea, leading to blindness. Transmission: often during birth or in children. Diagnosis: bacterial identification; treatment: antimicrobials, surgery for eyelid deformities.

Other Microbial Diseases of the Eye
Sties: Infection of sebaceous glands near the eye
Ophthalmia neonatorum: Conjunctival/corneal inflammation in newborns
Conjunctivitis (pink eye): Inflammation of conjunctiva
Keratitis: Inflammation of cornea
