 Back
BackMicrobial Diseases of the Respiratory System: Structure, Pathogenesis, and Clinical Features
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Chapter 24: Microbial Diseases of the Respiratory System
Structure and Function of the Respiratory System
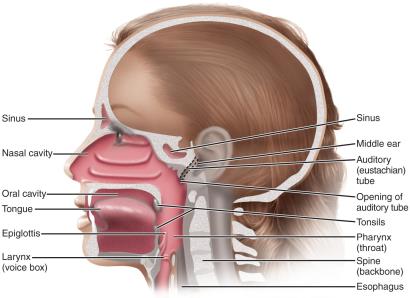
The respiratory system is divided into upper and lower regions, each with distinct anatomical structures and defense mechanisms against microbial invasion.
Upper respiratory system: Includes the nose, pharynx, middle ear, and eustachian tubes. Saliva and tears help protect mucosal surfaces from pathogens.
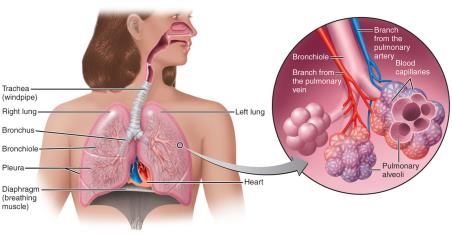
Lower respiratory system: Comprises the larynx, trachea, bronchial tubes, and alveoli. The ciliary escalator moves particles toward the throat, alveolar macrophages destroy microorganisms, and respiratory mucus provides additional protection.
Normal Microbiota of the Respiratory System
The respiratory tract harbors a variety of microorganisms, some of which are potentially pathogenic. The normal microbiota suppress pathogens by competing for nutrients and producing inhibitory substances. The lower respiratory system is nearly sterile due to these defense mechanisms.
Microbial Diseases of the Upper Respiratory System
Common Diseases and Their Features
Most upper respiratory diseases are self-limiting, but some can be severe or life-threatening.
Pharyngitis: Sore throat, often viral or bacterial in origin.
Laryngitis: Inflammation of the larynx.
Tonsillitis: Inflammation of the tonsils.
Sinusitis: Inflammation of the sinuses.
Epiglottitis: Most life-threatening; often caused by Haemophilus influenzae type b.
Bacterial Diseases of the Upper Respiratory System
Streptococcal pharyngitis (strep throat): Caused by group A streptococci (Streptococcus pyogenes), which are resistant to phagocytosis and produce streptokinases and streptolysins. Symptoms include local inflammation, fever, tonsillitis, and enlarged lymph nodes. Diagnosis is by throat culture or rapid antigen detection tests.
Scarlet fever: Results from erythrogenic toxin produced by lysogenized S. pyogenes.

Diphtheria: Caused by Corynebacterium diphtheriae (Gram-positive rod, pleomorphic). Begins with sore throat and fever, forms a tough grayish membrane in the throat, and produces an exotoxin that can damage the heart and kidneys. Treated with antibiotics and antitoxin; prevented by the DTaP vaccine.

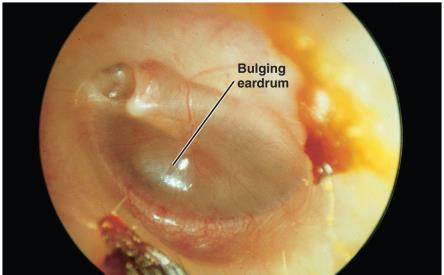
Otitis media: Infection of the middle ear, common in children. Caused by Streptococcus pneumoniae, nonencapsulated Haemophilus influenzae, Moraxella catarrhalis, S. pyogenes, and respiratory syncytial viruses. Treated with broad-spectrum penicillins.
The Common Cold
Caused by over 200 different viruses, including rhinoviruses, betacoronaviruses, mastadenoviruses, and enterovirus D68. Symptoms include sneezing, nasal secretion, and congestion, but usually no fever. Antibiotics are ineffective; treatment is symptomatic.
Microbial Diseases of the Lower Respiratory System
Overview
Diseases include bronchitis, bronchiolitis, and pneumonia, often caused by the same pathogens as upper respiratory infections. Pneumonia involves infection of the pulmonary alveoli.
Pertussis (Whooping Cough)
Caused by Bordetella pertussis (Gram-negative coccobacillus). The bacterium produces a capsule for attachment to ciliated cells, destroys these cells, and shuts down the ciliary escalator. The tracheal cytotoxin damages ciliated cells, and pertussis toxin causes systemic symptoms.
Stages:
Catarrhal stage: Resembles the common cold.
Paroxysmal stage: Violent coughing and gasping for air (1–6 weeks).
Convalescence stage: May last for months.
Prevention: DTaP vaccine.
Treatment: Erythromycin or other macrolides.

Tuberculosis
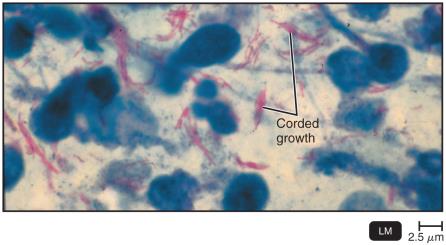
Caused by Mycobacterium tuberculosis (acid-fast rod, obligate aerobe). The bacterium's lipid-rich cell wall makes it resistant to drying and antimicrobials. Other causes include Mycobacterium bovis (bovine tuberculosis).
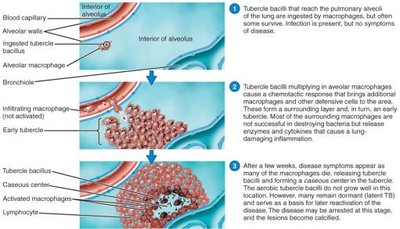
Pathogenesis of Tuberculosis
Inhaled organisms are phagocytized by alveolar macrophages.
Mycolic acids stimulate an inflammatory response, leading to the formation of tubercles (walled-off lesions).
Tubercles may heal and calcify (Ghon's complexes), resulting in latent TB (not infectious).
If immune defenses fail, tubercles break down, releasing bacteria and causing active, infectious TB or disseminated (miliary) TB.

Diagnosis and Treatment of Tuberculosis
Diagnosis: Tuberculin skin test (Mantoux), chest x-ray or CT, acid-fast staining, culture, rapid blood tests (γ-IFN), and nucleic acid amplification tests (NAAT).
Treatment: Minimum 6 months of drug therapy (isoniazid, rifampin, ethambutol, pyrazinamide). MDR and XDR strains require second-line drugs.
Vaccine: BCG (live, attenuated M. bovis), not widely used in the U.S.
Global Impact
10 million cases and 2 million deaths annually worldwide.
One-third of the world's population has latent TB.
Leading cause of death among HIV-infected individuals.
Bacterial Pneumonias
Typical pneumonia: Caused by Streptococcus pneumoniae.
Healthcare-associated pneumonia: Caused by Staphylococcus aureus.
Atypical pneumonia: Caused by other microorganisms, including mycoplasma.
Lobar pneumonia: Infects lung lobes; Bronchopneumonia: Infects alveoli adjacent to bronchi.
Pleurisy: Inflammation of pleural membranes.
Pneumococcal Pneumonia
Caused by S. pneumoniae (Gram-positive, encapsulated diplococci; 90 serotypes).
Infects bronchi/alveoli, causing fluid accumulation, fever, chest pain, and difficulty breathing.
Diagnosis: Optochin-inhibition test, bile solubility test, or capsular antigen in urine.
Treatment: Macrolides; Prevention: Conjugated pneumococcal vaccine (23 types).
Haemophilus influenzae Pneumonia
Gram-negative coccobacillus; symptoms resemble pneumococcal pneumonia.
Risk groups: Children under 5, adults over 65. Hib vaccine reduced incidence in children by 99%.
Diagnosis: Isolation on special media (X and V factors).
Treatment: Third-generation cephalosporins.
Mycoplasmal Pneumonia
Also called primary atypical or walking pneumonia; caused by Mycoplasma pneumoniae (no cell wall).
Mild but persistent symptoms; common in children and young adults.
Diagnosis: PCR; Treatment: Tetracyclines.

Legionellosis
Also called Legionnaires’ disease; caused by Legionella pneumophila (aerobic, gram-negative rod).
Grows in water systems, forms biofilms, survives in amebae. Transmitted by inhaling aerosols.
Symptoms: High fever, cough. Treatment: Azithromycin and macrolides.
Psittacosis (Ornithosis)
Caused by Chlamydia psittaci (gram-negative, obligate intracellular bacterium).
Transmitted from bird droppings via air. Symptoms: Fever, headache, chills, disorientation.
Diagnosis: Growth in eggs, cell culture, or PCR. Treatment: Tetracyclines.
Chlamydial Pneumonia
Caused by Chlamydia pneumoniae; transmitted person to person.
Mild respiratory illness, common in young people; possible association with atherosclerosis.
Diagnosis: PCR; Treatment: Azithromycin.
Q Fever
Caused by Coxiella burnetii (obligate intracellular gammaproteobacterium).
Transmitted to humans by inhalation of aerosols from animals or unpasteurized milk.
Symptoms: Acute (high fever, muscle aches, headache, cough); chronic (endocarditis).
Treatment: Doxycycline; chloroquine for chronic infections.
Viral Diseases of the Respiratory System
Viral Pneumonia
Often a complication of influenza, measles, or chickenpox. Coronaviruses have caused several major respiratory syndromes, including SARS, MERS, and COVID-19.
COVID-19
Caused by Betacoronavirus SARS-CoV-2; first reported in December 2019 in China.
Declared a pandemic in March 2020; by December 2022, 667 million infections and 7 million deaths worldwide.
Classification and Description of SARS-CoV-2
Sense (+) strand RNA genome bound to nucleoprotein; envelope contains spike (S), membrane (M), and envelope (E) proteins.
High mutation rate leads to antigenic drift and emergence of variants.
Signs and Symptoms of COVID-19
Range from minor to life-threatening; risk factors include age, chronic diseases, and immunocompromised states.
Symptoms: Fever, cough, shortness of breath, fatigue, loss of smell/taste, gastrointestinal symptoms.
"Long COVID" (PASC): Persistent symptoms such as fatigue and cognitive difficulties.
Transmission: Primarily airborne; individuals are infectious before and after symptom onset.
Diagnosis: Home ELISA antigen tests, PCR for viral RNA.
Treatment: Remdesivir, Paxlovid, molnupiravir, convalescent plasma.
Vaccines: mRNA, virus-vector, and subunit vaccines targeting the spike protein.
Respiratory Syncytial Virus (RSV)
Most common viral respiratory disease in infants; can cause life-threatening pneumonia in infants and older adults.
Diagnosis: Serological tests; Treatment: Palivizumab; vaccines under development.
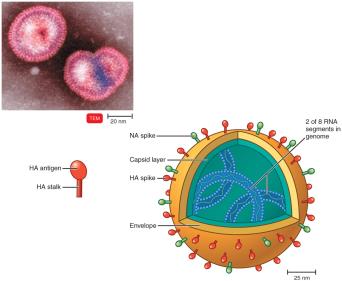
Influenza (Flu)
Caused by Influenzavirus; contains eight RNA segments, protein capsid, and envelope with HA and NA spikes.
Symptoms: Chills, fever, headache, muscle aches; no intestinal symptoms.
Antigenic drift (minor changes) and antigenic shift (major changes) allow evasion of immunity and can lead to pandemics.
Three genera: Influenza A (most variable, causes pandemics), B (seasonal epidemics), and C.
Diagnosis: Rapid antigen tests, PCR; Treatment: Zanamivir, oseltamivir; Prevention: Annual multivalent vaccine.
Fungal Diseases of the Respiratory System
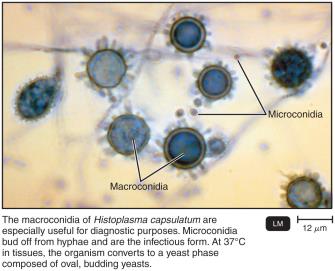
Histoplasmosis
Caused by Histoplasma capsulatum (dimorphic fungus); yeast form grows in macrophages.
Acquired from airborne conidia in areas with bird or bat droppings; treated with itraconazole.
Coccidioidomycosis (Valley Fever)
Caused by Coccidioides immitis (dimorphic fungus); found in desert soils of the American Southwest.
Forms spherules with endospores in tissues; most infections are mild, but some resemble tuberculosis.
Treatment: Fluconazole or itraconazole.
Pneumocystis Pneumonia (PCP)
Caused by Pneumocystis jirovecii (yeast-like fungus); asymptomatic in immunocompetent, but causes pneumonia in immunocompromised (AIDS indicator).
Treatment: Trimethoprim-sulfamethoxazole.
Blastomycosis
Caused by Blastomyces dermatitidis (dimorphic fungus); grows in soil.
Symptoms: Resemble bacterial pneumonia, cutaneous abscesses, tissue damage.
Treatment: Itraconazole and amphotericin B.
Other Fungi Involved in Respiratory Disease
Aspergillus fumigatus: Causes aspergillosis; grows in compost piles.
Rhizopus and Mucor: Mold spores; risk factors include immunocompromised state, cancer, and diabetes.
