 Back
BackMicrobial Diseases of the Skin and Wounds: Bacterial Infections
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Microbial Diseases of the Skin and Wounds
Structure and Function of the Skin
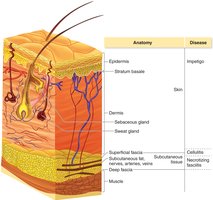
The skin is the largest organ of the human body and serves as a critical barrier against microbial invasion. It is composed of two main layers: the epidermis (outer layer) and the dermis (inner layer). The skin prevents excessive water loss, regulates temperature, is involved in sensory phenomena, assists in vitamin D formation, and acts as a barrier to pathogens.
Microbiome of the Skin
The skin hosts a diverse microbiome, including bacteria and yeasts, which are typically harmless and compete with potential pathogens for nutrients and space. These microbes are difficult to remove completely and are most abundant in moist areas. Waste products from these microbes can cause body odor. Common genera include Staphylococcus, Micrococcus, and diphtheroids, as well as the yeast Malassezia. Opportunistic infections can occur if the skin barrier is breached or the immune system is compromised.
Bacterial Diseases of the Skin and Wounds
Folliculitis
Folliculitis is an infection of the hair follicle, often presenting as a pimple. When it occurs at the base of the eyelid, it is called a sty. If the infection spreads, it can form furuncles (boils), and when multiple furuncles coalesce, they form carbuncles.
Etiology: Most commonly caused by Staphylococcus species, especially S. aureus and S. epidermidis.
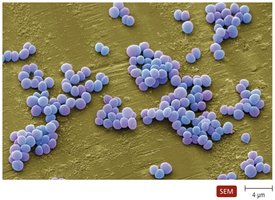
Characteristics: Gram-positive cocci, arranged in clusters, facultatively anaerobic, tolerant of salt and desiccation.



Staphylococcus Species
S. epidermidis: Common on the skin, lacks major virulence factors, rarely causes disease.
S. aureus: Transiently colonizes skin and mucous membranes, more virulent.
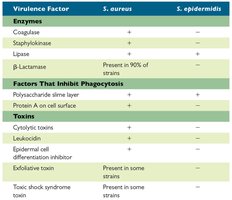
Virulence Factors of Staphylococcus
Virulence Factor | S. aureus | S. epidermidis |
|---|---|---|
Coagulase | + | – |
Staphylokinase | + | – |
Lipase | + | + |
β-Lactamase | Present in 90% of strains | – |
Polysaccharide slime layer | + | + |
Protein A on cell surface | + | – |
Cytolytic toxins | + | – |
Leukocidin | + | – |
Epidermal cell differentiation inhibitor | Present in some strains | – |
Exfoliative toxin | Present in some strains | – |
Toxic shock syndrome toxin | Present in some strains | – |
Pathogenesis and Epidemiology
Transmitted via direct contact or fomites.
Infection can spread to the blood and internal organs.
Treatment and Prevention
Diagnosis: Isolation of Gram-positive cocci in clusters from pus.
Treatment: Mupirocin or dicloxacillin; vancomycin for resistant strains.
Prevention: Hand hygiene and proper hospital procedures to minimize MRSA infections.
Staphylococcal Scalded Skin Syndrome (SSSS)
SSSS is caused by certain strains of S. aureus that produce exfoliative toxins. It is characterized by red, wrinkled skin that forms blisters and peels off in sheets. The dermis is unaffected, so no scarring occurs. Most cases occur in infants and are transmitted person-to-person.



Diagnosis: Characteristic sloughing of skin.
Treatment: Antimicrobial drugs.
Prevention: Difficult due to widespread presence of S. aureus.
Impetigo (Pyoderma) and Erysipelas
Impetigo presents as red patches on the face and limbs, while erysipelas involves infection spreading to lymph nodes. Most cases are caused by S. aureus, with some due to Streptococcus pyogenes. Virulence factors include M protein, hyaluronic acid, and pyrogenic toxins.


Pathogenesis: Bacteria invade compromised skin; can lead to acute glomerulonephritis if kidneys are affected.
Epidemiology: Transmitted by contact or fomites; impetigo common in children, erysipelas in the elderly.
Diagnosis: Presence of vesicles is diagnostic for impetigo.
Treatment: Oral/topical antimicrobials for impetigo; penicillin for erysipelas.
Prevention: Good hygiene and cleanliness.
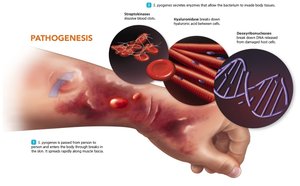
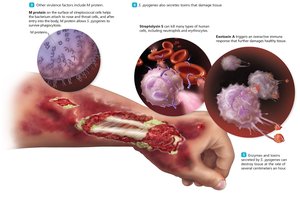
Necrotizing Fasciitis
Necrotizing fasciitis is a rapidly progressing infection causing redness, intense pain, swelling, and tissue destruction. Most cases are due to Streptococcus pyogenes, with some caused by S. aureus. Virulence factors include enzymes and toxins (exotoxin A, streptolysin S) that facilitate tissue invasion and destruction.

Epidemiology: Usually spread person-to-person; mortality rate ~20%.
Diagnosis: Difficult early due to nonspecific symptoms.
Treatment: Clindamycin and penicillin; surgical debridement often required.
Prevention: Difficult due to common presence of S. pyogenes.
