 Back
BackMicrobial Diseases of the Skin and Eyes: Structure, Pathogenesis, and Clinical Manifestations
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Diseases of the Skin and Eyes
Introduction
The skin and eyes serve as important barriers against microbial invasion. However, various microorganisms can overcome these defenses, leading to a range of infectious diseases. This chapter explores the structure of the skin, its protective mechanisms, and the major microbial diseases affecting the skin and eyes, including their causative agents, pathogenesis, clinical features, and treatments.
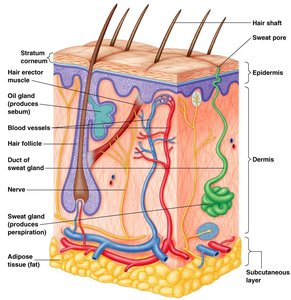
Skin: Structure and Protective Properties
Physical and Chemical Barriers
Skin is composed of multiple layers, including the epidermis, dermis, and subcutaneous tissue, providing a physical barrier to pathogens.
Properties that inhibit microbial growth include:
High salt concentration (from sweat)
Dryness
Low pH (acidic environment)
Presence of lysozyme, an enzyme that hydrolyzes peptidoglycan in bacterial cell walls
Normal microbiota of the skin includes Gram-positive, salt-tolerant bacteria such as Staphylococci, Micrococci, and diphtheroids.
Mucous Membranes
Line body cavities open to the exterior (e.g., eyes, mouth).
Cells secrete mucus, trapping foreign invaders.
Some cells possess cilia, which move mucus and trapped particles out of the body (ciliary escalator).
Common Signs and Symptoms of Skin Diseases
Rashes and Lesions
Exanthem: Skin rash arising from disease conditions.
Enanthem: Rash on mucous membranes (e.g., inside the mouth).
Lesions: Abnormal changes in tissue structure, often containing fluid or pus.
Pus: Protein-rich fluid containing dead leukocytes and cellular debris, often present in bacterial infections.


Bacterial Infections of the Skin
Staphylococcal Infections
Staphylococcus epidermidis: Gram-positive, normal flora, opportunistic pathogen.
Staphylococcus aureus: Gram-positive, often found in nasal passages, most pathogenic of staphylococci, major cause of nosocomial infections.
Produces toxins such as leukocidins, hemolysins, exfoliative toxin (causes scalded-skin syndrome), and enterotoxins (affect GI tract).
Coagulase-positive strains can clot fibrin in blood.
Antibiotic-resistant strains (e.g., MRSA) are a significant concern.
Clinical Manifestations
Folliculitis: Infection of hair follicles.
Sty (stye): Folliculitis of an eyelash.
Furuncle: Abscess/boil; localized region of pus surrounded by inflamed tissue.
Carbuncle: Inflammation of tissue under the skin, can lead to systemic illness.
Impetigo: Highly contagious skin infection, primarily in children.
Scalded Skin Syndrome (SSS): Toxin-mediated separation of skin layers.
Toxic Shock Syndrome (TSS): Caused by TSST-1 superantigen, leading to massive cytokine release, shock, and potentially death.


MRSA (Methicillin-Resistant Staphylococcus aureus)
HA-MRSA: Hospital-acquired, serious in immunocompromised patients.
CA-MRSA: Community-acquired, more virulent, can affect healthy individuals.
Secretes modulins, peptides that recruit and destroy neutrophils.
Streptococcal Infections
Streptococcus pyogenes: Gram-positive, grows in chains, catalase-negative, Group A Streptococcus (GAS).
Virulence factors include:
Hemolysins (alpha, beta, gamma) – destroy red blood cells.
Leukocidins – destroy leukocytes.
M protein – antiphagocytic, aids in adherence, antigenic variation, degrades complement protein C3b.
Streptokinases – dissolve blood clots.
Streptococcal pyrogenic exotoxins (SPEs) – superantigens causing fever and hypersensitivity responses (e.g., scarlet fever, STSS).
Hyaluronidase – dissolves connective tissue.

Clinical Manifestations
Erysipelas: Erythema affecting the dermal layer, sometimes involving lymphatics.
Impetigo: Also caused by Streptococcus pyogenes.
Necrotizing fasciitis: Rapidly progressing infection resulting in death of soft tissue, can be fatal.



Pseudomonas Infections
Pseudomonas aeruginosa: Gram-negative, aerobic rod, produces blue-green pus (pyocyanin).
Common in swimming pools, hot tubs, and as a nosocomial infection, especially in burn patients.
Can cause Pseudomonas dermatitis and otitis externa (swimmer’s ear).
Propionibacterium Infections (Acne)
Propionibacterium acnes: Gram-positive, anaerobic rod.
Comedonal (mild) acne: Blocked sebum channels.
Inflammatory acne: Infection by P. acnes, which metabolizes glycerol in sebum.
Treatment: Antibiotics, benzoyl peroxide, visible (blue) light therapy.

Viral Infections of the Skin
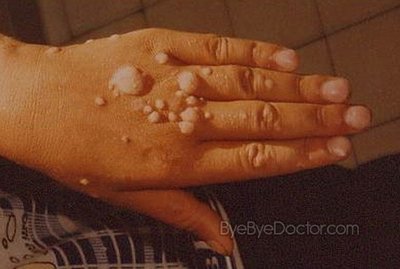
Papillomaviruses (HPV)
Over 50 types; cause warts (verrucae).
Transmitted by contact; some types (e.g., HPV-16) are associated with cancers (cervical, anal, oral, etc.).
Vaccine available, significantly reduces cervical cancer risk.
Epidermodysplasia verruciformis: "Tree man" disease, rare genetic susceptibility to HPV.

Poxviruses
Smallpox (variola virus): Transmitted via respiratory route, causes ulcers, macular rash, fever.
Variola major (~20% mortality), variola minor (<1% mortality).
First disease with a vaccine (Edward Jenner, 1796).
Monkeypox: Zoonotic, milder than smallpox, recent outbreaks.
Herpesviruses
Varicella-zoster virus (HHV-3): Causes chickenpox (varicella) and shingles (zoster).
Transmitted via respiratory route; virus remains latent in dorsal root ganglion.
Reactivation causes shingles, which can lead to Ramsay-Hunt syndrome (facial paralysis).
Vaccine available.
HSV-1: Oral herpes (cold sores, blisters).
HSV-2: Genital herpes.
Other manifestations: Herpes gladiatorum (skin), herpes whitlow (fingers), herpes encephalitis (brain infection, high fatality).
Treatment: Antivirals such as acyclovir.
Measles (Rubeola) and German Measles (Rubella)
Measles virus: Causes Koplik’s spots (enanthem in mouth), macular rash, fever; highly contagious via respiratory route.
Can cause immune amnesia and encephalitis (1/1,000 cases).
Vaccine: MMR (measles, mumps, rubella).
Rubella virus: Causes milder macular rash and fever; congenital rubella syndrome can cause severe fetal damage.
Other Viral Exanthems
Parvovirus B19: Erythema infectiosum (fifth disease), "slapped cheek" rash.
HHV-6 and HHV-7: Roseola (sixth disease), high fever followed by rash.
Fungal Infections of the Skin
Cutaneous Mycoses
Fungi that metabolize keratin, causing dermatomycoses (tineas or ringworm).
Common genera: Trichophyton (hair, skin, nails), Epidermophyton (skin, nails), Microsporum (hair, skin).
Treatment: Oral griseofulvin, topical miconazole.
Subcutaneous Mycoses
Sporotrichosis: Caused by Sporothrix schenckii, enters via puncture wounds ("rose handler’s disease").
Can cause nodular lesions, may spread to joints, bones, CNS if untreated.
Treatment: Potassium iodide (KI).
Candidiasis
Candida albicans: Causes oral thrush (white patches, soreness), urogenital yeast infections (itching, discharge).
Risk factors: Antibiotic therapy, immunosuppression.
Treatment: Miconazole, nystatin, fluconazole (Diflucan).
Arthropod Infections of the Skin
Scabies
Caused by Sarcoptes scabiei (mite), which burrows in the skin to lay eggs.
Symptoms: Itching, rash.
Transmission: Contact, fomites (clothes, bedding, furniture).
Treatment: Topical insecticides.
Pediculosis (Lice)
Caused by Pediculus humanus capitis (head louse).
Symptoms: Itching, mild reaction to bites, swollen lymph nodes.
Transmission: Contact; lice feed on blood and lay eggs (nits) on hair.
Treatment: Topical insecticides, removal of eggs.
Bacterial Infections of the Eyes
Conjunctivitis (Pinkeye)
Most commonly caused by Haemophilus influenzae, but various microbes can be responsible.
Symptoms: Swelling of conjunctiva, red eyes.
Transmission: Contact, unsanitary conditions (e.g., poor hand hygiene, unsanitary contact lens use).
Treatment: Topical antibiotics.
Ophthalmia Neonatorum
Caused by Neisseria gonorrhoeae, transmitted to newborns during birth.
Can lead to blindness if untreated; previously prevented with silver nitrate, now with antibiotics.
Inclusion Conjunctivitis and Trachoma
Caused by Chlamydia trachomatis.
Inclusion conjunctivitis: Inflammation, transmitted during birth or via contaminated water.
Trachoma: Chronic infection, roughens inner eyelid, causes corneal scarring and blindness; leading cause of infectious blindness worldwide.
Transmission: Arthropods (flies), fomites (towels).
Treatment: Tetracycline.
Protozoan Infections of the Eyes
Acanthamoeba Keratitis
Caused by Acanthamoeba species, found in freshwater.
Slowly destroys the cornea, leading to blindness.
Risk factors: Unsanitary contact lenses, cleaning lenses with tap water.
