 Back
BackMicrobial Diseases of the Skin: Structure, Pathogenesis, and Clinical Manifestations
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Infections of the Skin
Skin Anatomy
The skin is the body's largest organ and serves as a primary barrier against microbial invasion. It is composed of two main layers:
Epidermis: The most superficial layer, consisting of several sublayers. The outermost layer, the stratum corneum, is rich in keratin and dead cells, providing a tough, protective barrier.
Dermis: A deeper, thicker layer made mostly of connective tissue. It contains glands, hair follicles, and supports the epidermis.
Descriptions of Skin Infections
Diagnosis of skin infections often begins with careful observation of the lesion's appearance. Common lesion types include:
Vesicle: A small, fluid-filled lesion (<1 cm).
Bulla (pl. bullae): A larger, fluid-filled lesion (>1 cm).
Pustule: A pus-filled lesion.
Macule: A flat, reddened lesion.
Papule: A raised, reddened lesion.

Bacterial Skin Infections
General Overview
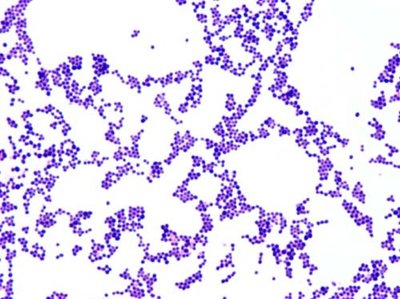
Bacterial skin infections are most commonly caused by the genera Staphylococcus and Streptococcus. These bacteria can produce invasive enzymes and toxins that damage host tissues.
Staphylococcal Skin Infections
Staphylococci: Gram-positive cocci, can be coagulase-positive or coagulase-negative.
Coagulase-negative: S. epidermidis is common skin flora, usually pathogenic only if the skin is broken.
Coagulase-positive: S. aureus is the most pathogenic species, producing coagulase (an enzyme that forms clots).

Staphylococcus aureus: Pathogenic Mechanisms
Carried by about 20% of the population in the nose.
Can survive for months on surfaces.
Produces a yellow pigment that protects against sunlight.
Induces strong inflammatory responses and attracts immune cells.
Has multiple mechanisms to evade host defenses, including blocking chemotaxis, killing phagocytes, resisting lysozyme, and evading opsonization.
Antibodies are not effective in preventing reinfection.
Clinical Manifestations of Staphylococcal Infections
Impetigo: Highly contagious, common in children (2-5 years), presents as isolated pustules that become crusted. Can be caused by Staph or Strep.
Scalded Skin Syndrome: Caused by exfoliative toxin B, leading to separation and shedding of skin layers. Associated with toxic shock syndrome (TSS).




Folliculitis: Infection of hair follicles, causing pimples or sties (if on the eyelid). More severe forms include furuncles (boils) and carbuncles, which may be accompanied by systemic symptoms like fever.
Toxic Shock Syndrome (TSS): Characterized by fever, vomiting, rash, shock, and possible organ failure. Caused by superantigenic toxins; can be menstrual or non-menstrual.
Streptococcal Skin Infections
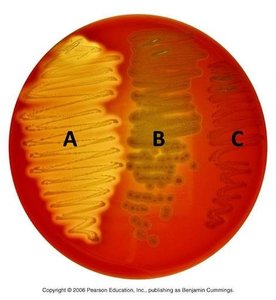
Streptococci: Gram-positive cocci that secrete toxins and enzymes. Classified by hemolysin production:
Alpha-hemolytic: Partial hemolysis, green halos (e.g., S. mutans).
Beta-hemolytic: Complete hemolysis, clear halos (e.g., S. pyogenes).
Gamma-hemolytic: Non-hemolytic.
Streptococcus pyogenes (Group A Streptococcus, GAS)
Beta-hemolytic, highly virulent, causes a variety of diseases.
Has M protein to prevent phagocytosis.
Produces streptolysins (lyse RBCs, toxic to neutrophils), streptokinases (dissolve clots), and hyaluronidase (breaks down connective tissue).
Clinical Manifestations of Streptococcal Infections
Erysipelas: Reddish patches with raised margins, usually starting on the face. Can cause local tissue destruction and sepsis; high fever is common.
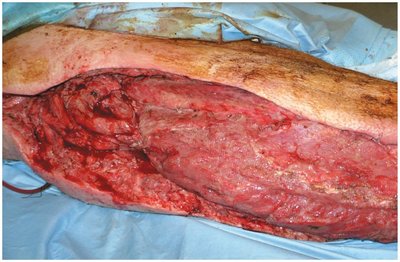
Necrotizing Fasciitis: "Flesh-eating bacteria" infection that rapidly destroys tissue. Mortality rates can exceed 40%.


Pseudomonas aeruginosa
Gram-negative rod, survives in moist environments (e.g., soap films, mop water, flower vases).
Model opportunistic pathogen, especially dangerous for cystic fibrosis and burn patients (produces blue-green pus).
Can cause dermatitis, folliculitis, and swimmer's ear in hot tubs and pools.
Highly resistant to many antibiotics and disinfectants.
Clostridium perfringens
Gram-positive, anaerobic rod, common in the environment.
Causes gas gangrene: death of soft tissue due to ischemia (lack of blood supply), which creates an anaerobic environment for bacterial growth.
Bacteria ferment carbohydrates, producing gases that swell tissue, and secrete toxins/enzymes that degrade tissue.
Treatment: Amputation is most common; hyperbaric oxygen therapy may be used when amputation is not possible.


Acne
One of the most common skin conditions, affecting millions.
Results from increased shedding of skin cells and sebum production, leading to clogged follicles.
Comedonal acne: Whiteheads and blackheads; treated topically.
Inflammatory acne: Caused by Propionibacterium acnes metabolizing sebum, triggering inflammation; treated by reducing sebum and using antibiotics.
Nodular cystic acne: Severe form with nodules or cysts, often resulting in scarring.


Viral Infections of the Skin
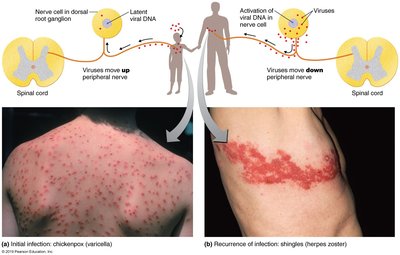
Chickenpox (Varicella)
Caused by Varicella-zoster virus (human herpesvirus-3).
Entry via respiratory tract; virus hides in peripheral nerves, evading antibodies.
Humans are the only known reservoir.
Initial infection presents as a vesicular skin rash; complications in adults include pneumonia and encephalitis.
Dangerous for pregnant women (risk of miscarriage, birth defects).
Prevented by an attenuated vaccine.

Shingles (Herpes Zoster)
Reactivation of latent varicella-zoster virus, often due to stress or immunosuppression.
Vesicular rash typically appears on one side of the body, following a peripheral nerve.
Rash is painful and may persist as postherpetic neuralgia.
Vaccine (higher dose of chickenpox vaccine) recommended for adults over 60.

Human Herpes Simplex Virus Type I (HSV-1)
Causes fever blisters/cold sores (herpes labialis), transmitted via saliva and respiratory routes.
Virus remains latent in the trigeminal nerve ganglion; reactivation triggered by fever, sunlight, stress, or menstruation.
No cure, but antivirals can reduce symptoms.
Other manifestations: Herpes gladiatorum (skin, common in wrestlers), Herpes whitlow (fingers, especially in healthcare workers).


Measles (Rubeola)
Caused by the rubeola virus (RNA, enveloped); humans are the only reservoir.
Highly contagious, transmitted by inhalation; infectious before symptoms appear.
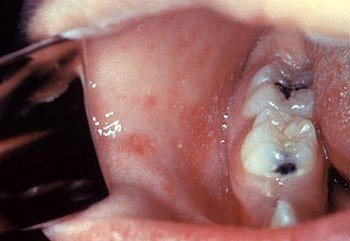
Symptoms: Macular rash starting on the face, spreading to trunk and extremities; Koplik spots (white spots on mucous membranes) are diagnostic.
Complications: Encephalitis (1/1000 cases), high mortality in children under 1 year.
Prevention: MMR vaccine.


Rubella (German Measles)
Caused by the rubella virus, transmitted by inhalation.
Symptoms: Macular rash (usually starts on the face), mild fever.
Pregnant women: Risk of congenital rubella syndrome (35% chance of serious fetal damage, including deafness, cataracts, heart defects, mental retardation, autism, and death).
Vaccination of women of childbearing age is crucial.
Smallpox (Variola)
Caused by the variola virus (major and minor strains).
Symptoms: Fever, headache, nausea, vomiting, followed by a pustular rash starting in the mouth and spreading to the body.
High mortality (20-60% for major strain); eradicated worldwide in 1977.
Vaccine exists but does not provide long-term immunity and carries risks.
Potential bioterrorism threat.
Warts
Caused by papillomaviruses; benign tumors called papillomas.
Spread by direct contact or fomites; plantar warts occur on the soles of the feet.
Most warts resolve spontaneously within 2-5 years.
Certain types can lead to skin or cervical cancer.
Fungal Infections (Mycoses)
Dermatophytes
Fungi that colonize hair, nails, and the outer layer of skin.
Produce enzymes that digest keratin.
Common infections (tinea):
Tinea pedis: Athlete's foot
Tinea capitis: Ringworm of the scalp
Tinea unguium (onychomycosis): Nails
Tinea cruris: Jock itch (groin)
Not life-threatening; treated with topical antifungals.
