 Back
BackMicrobial Infections of the Genitourinary System: Structure, Pathogenesis, and Clinical Syndromes
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Genitourinary System: Structure and Normal Biota
Overview of the Genitourinary Tract
The genitourinary tract consists of two distinct organ systems: the urinary tract and the genital (reproductive) system. Both systems are susceptible to microbial infections, which can lead to significant morbidity.
Urinary tract: Removes substances from the blood, regulates body processes, forms urine, and transports it out of the body.
Genital system: Primarily functions in reproduction; includes male and female reproductive organs.
Normal Biota of the Genitourinary Tract
Outer urethra: Harbors some normal biota in both genders.
Male genital tract: The urethra contains some normal flora; other organs are typically sterile.
Female genital tract: The vagina contains a normal population of microbes; above the cervix, organs are sterile.
Urine flow: Helps maintain sterility in the urinary tract, but urine can support microbial growth if introduced.
Urinary Tract Infections (UTIs)
Types and Clinical Manifestations
UTIs result from the invasion of the urinary system by bacteria or other microorganisms. They are among the most common healthcare-associated infections.
Cystitis: Infection of the urinary bladder, often with sudden onset of pain, frequent urges to urinate, dysuria (burning pain), cloudy urine, hematuria (blood in urine), low-grade fever, and nausea.
Pyelonephritis: Infection of the kidneys, presenting with back pain and high fever; can cause permanent kidney damage if untreated.
Urethritis: Infection limited to the urethra.

Etiology and Epidemiology
Most common cause: Escherichia coli (80% of cases), originating from the gastrointestinal tract.
Transmission: Not person-to-person; bacteria ascend from the GI tract to the urinary system.
Risk factors: Female anatomy (short urethra, proximity to anus), urinary catheters, reduced urine flow.
Treatment: Antibiotics are the mainstay of therapy.
Reproductive Tract Diseases Caused by Microorganisms
Sexually Transmitted Infections (STIs) and Discharge Diseases
Many reproductive tract diseases are sexually transmitted. Discharge diseases are characterized by increased fluid discharge from the reproductive tract, facilitating transmission.
Common discharge diseases: Gonorrhea, Chlamydia, Trichomoniasis.
Impact: Responsible for high rates of infertility and reproductive complications.
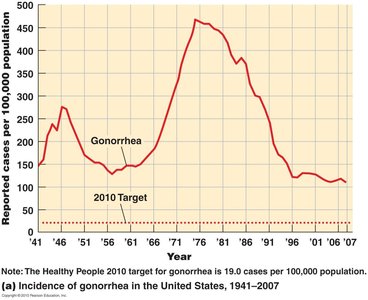
Gonorrhea
Causative agent: Neisseria gonorrhoeae, transmitted via sexual contact.
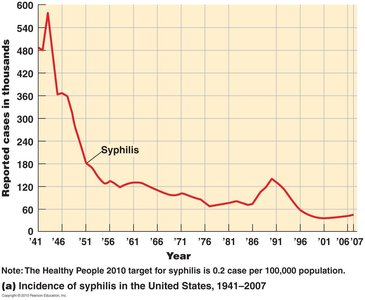
Incidence: High in the U.S.; see epidemiological trends below.
Signs and symptoms in males: Urethritis, painful urination, yellowish discharge, possible asymptomatic cases, risk of infertility due to scarring.
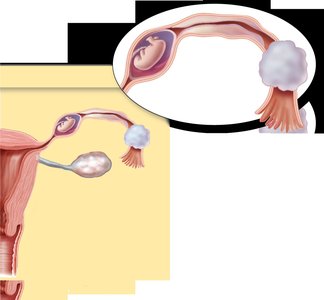
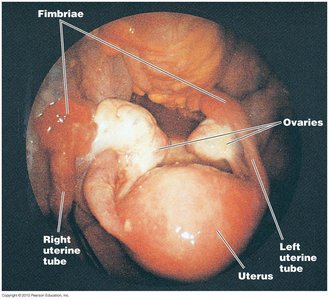
Signs and symptoms in females: Mucopurulent or bloody vaginal discharge, painful urination, risk of ascending infection (uterus, fallopian tubes), serious neonatal eye infections if transmitted during birth.

Complications: Salpingitis (fallopian tube inflammation), pelvic inflammatory disease (PID), infertility, ectopic pregnancy.
Prevention: No vaccine; condoms are effective.
Treatment: Antibiotics.
Chlamydia
Causative agent: Chlamydia trachomatis; most common reportable infectious disease in the U.S.
Prevalence: Higher than gonorrhea; most cases are asymptomatic.
Signs and symptoms in males: Urethritis, discharge, painful urination, risk of epididymitis.
Signs and symptoms in females: Cervicitis, discharge, salpingitis, high risk of PID, risk of neonatal conjunctivitis.
Prevention: Abstinence, barrier protection (condoms), annual screening for young women.
Treatment: Antibiotics.
Vaginitis and Vaginosis
Vaginitis: Inflammation of the vagina, often with itching, burning, and discharge.
Vaginosis: Similar to vaginitis but without significant inflammation.
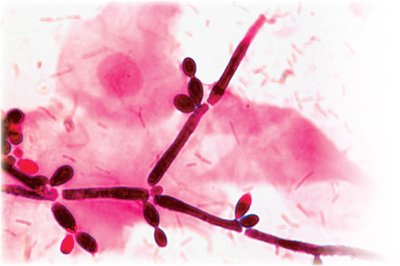
Candida albicans (Yeast Infection)
Causative agent: Candida albicans, a common yeast and normal biota in humans.
Symptoms: Itching, burning, thick white discharge.
Diagnosis: Wet prep or Gram stain of vaginal material.
Transmission: Usually opportunistic; risk factors include antibiotics, diabetes, pregnancy.
Treatment: Topical and oral antifungals (e.g., miconazole).

Bacterial Vaginosis (Gardnerella species)
Causative agent: Gardnerella species.
Symptoms: Fishy-smelling discharge, itching, little inflammation.
Complications: PID, infertility, ectopic pregnancy.
Transmission: Not strictly sexually transmitted; associated with sexual activity.
Trichomoniasis
Causative agent: Trichomonas vaginalis, a protozoan.
Symptoms: Often asymptomatic; females may have frothy, white to green discharge.
Transmission: Sexual contact; common nonviral STI.
Genital Ulcer Diseases
Syphilis
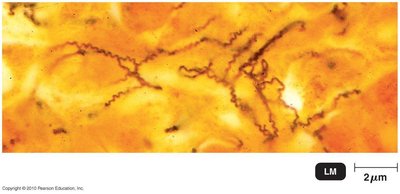
Causative agent: Treponema pallidum, a spirochete bacterium.
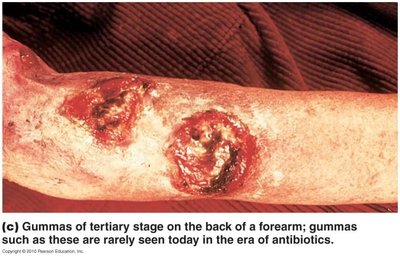
Stages: Primary (chancre), secondary (rash, systemic symptoms), tertiary (gummas, cardiovascular/neurological symptoms).


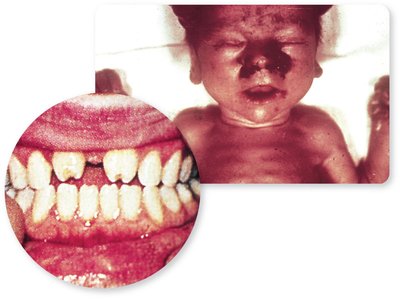
Congenital syphilis: Transmission from mother to fetus; can cause miscarriage, stillbirth, bone/nervous system defects, Hutchinson's teeth.
Prevention: Barrier protection (condoms); no vaccine.
Treatment: Antibiotics (e.g., penicillin).
Genital Herpes
Causative agents: Herpes simplex virus type 1 (HSV-1) and type 2 (HSV-2).
Symptoms: Painful vesicles on genitalia, malaise, fever, recurrent episodes possible.
Transmission: Direct contact with secretions; can occur without visible lesions.
Prevalence: Very common; many cases are unrecognized.
Prevention: No vaccine yet; condoms provide partial protection.
Treatment: Antivirals (e.g., acyclovir) reduce symptoms and viral shedding.

Wart Diseases of the Genital Tract
Human Papillomavirus (HPV) Infection
Causative agent: Human papillomavirus (HPV); multiple types, some oncogenic.
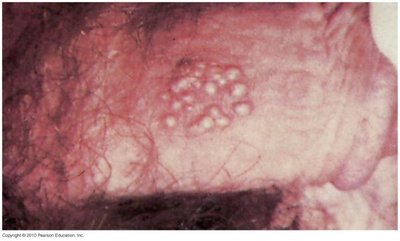
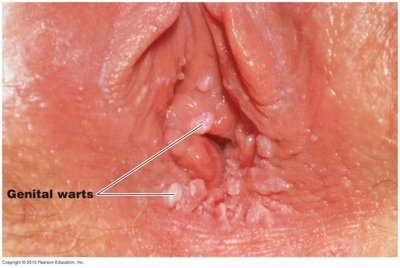
Symptoms: Genital warts (condyloma acuminata), flat or cauliflower-like masses; can be asymptomatic.
Complications: Cervical, penile, anal, and oropharyngeal cancers; five types (HPV-16, -18, -31, -33, -35) are high-risk for cervical cancer.
Prevalence: Highest in young women; 25–46% of women under 25 infected.
Prevention: Gardasil vaccine (protects against four types), barrier protection, regular Pap smears for cervical screening.
Treatment: Warts can be removed, but infection is incurable; virus may persist or resolve unpredictably.


Molluscum Contagiosum
Causative agent: Unclassified virus in the Poxviridae family.
Symptoms: Wartlike growths on genital mucosa or skin; usually benign except in immunocompromised individuals.
Transmission: Sexual contact, fomites (clothing, towels), autoinoculation.
Group B Streptococcus "Colonization"—Neonatal Disease
Agent: Beta-hemolytic Streptococcus, Lancefield group B.
Colonization: 10–40% of women are asymptomatic carriers; risk to neonates during birth.
Neonatal complications: Bloodstream infections, meningitis, pneumonia, possible permanent disabilities.
Prevention: CDC recommends screening at 35–37 weeks of pregnancy; positive women treated with antibiotics before delivery.

