 Back
BackMicrobiology of Skin Infections: Pathogens, Syndromes, and Clinical Management
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Skin Infections: Overview and Learning Goals
Introduction to Skin Pathogens
Skin infections are caused by a diverse group of microorganisms, including bacteria, viruses, fungi, protozoa, and helminths. Understanding the syndromes, causative agents, epidemiology, transmission, diagnosis, treatment, and prevention is essential for effective clinical management.
Syndromes: Range from superficial rashes to life-threatening systemic diseases.
Pathogens: Include bacteria (e.g., Staphylococcus aureus, Streptococcus pyogenes), viruses (e.g., measles, varicella-zoster), fungi (e.g., dermatophytes), protozoa, and helminths.
Transmission: Often via direct contact, respiratory droplets, or fomites.
Diagnosis and Treatment: Based on clinical presentation, laboratory tests, and antimicrobial therapy.
Classification of Skin Pathogens
Major Groups of Human Pathogens
Helminths: Parasitic worms such as tapeworms (Taenia spp.), flukes (Schistosoma), and nematodes (e.g., Ascaris).
Protozoa: Single-celled eukaryotes including Entamoeba, Giardia, Leishmania, and Plasmodium.
Fungi: Yeasts (e.g., Candida), molds (e.g., Aspergillus), and dermatophytes (e.g., Microsporum).
Bacteria: Gram-positive (e.g., Staphylococcus, Streptococcus), Gram-negative (e.g., Neisseria, Pseudomonas), and others (e.g., Mycobacterium).
Viruses: DNA viruses (e.g., herpesviruses, poxviruses) and RNA viruses (e.g., measles, rubella, influenza).
Arthropods: Vectors such as ticks, lice, mites, mosquitoes, and fleas.
Skin Immunity and Defense Mechanisms
Innate Immune Features of the Skin
The skin provides a robust barrier to infection through physical, chemical, and biological mechanisms:
Melanin: Possesses antimicrobial properties.
Perspiration: Acidic pH, high salt content, and mechanical washing action remove microbes.
Lysozyme: Enzyme that degrades bacterial cell walls.
Sebum: Oily secretion with low pH; metabolized by skin bacteria to produce toxic fatty acids.
Skin Lesions: Classification and Clinical Relevance
Primary and Secondary Lesions
Skin lesions are classified as primary (initial presentation) or secondary (evolution of primary lesions or due to external factors):
Primary lesions: Vesicles, bullae, macules, papules, pustules, cysts, and nodules.
Secondary lesions: Crusts, scales, purpura, petechiae, ulcers.


Viral Exanthems and Enanthems
Definitions and Clinical Syndromes
Exanthems are widespread rashes that appear abruptly, often in childhood, and are associated with viral infections, toxins, or immune responses. Enanthems are mucous membrane eruptions that often accompany exanthems and aid in diagnosis (e.g., Koplik spots in measles).
Major childhood exanthems: Measles, Scarlet fever, Rubella, Erythema infectiosum, Roseola.
Common features: Person-to-person aerosol transmission, human reservoir, skin rash involvement.
Measles (Rubeola)
Measles is a highly contagious viral disease caused by a single-stranded, negative-sense RNA virus (family Paramyxoviridae). Transmission occurs via respiratory droplets.
Incubation: 10-14 days.
Prodrome: Fever, malaise, conjunctivitis, cough, coryza, photophobia.
Enanthem: Koplik spots (bluish-gray specks on red base, buccal mucosa).
Exanthem: Maculopapular rash starting on face, spreading to trunk and extremities.
Complications: Subacute sclerosing panencephalitis (SSPE), pneumonia, otitis media.
Diagnosis: Clinical signs, viral antigen detection.
Treatment: Supportive; no antiviral drugs.
Prevention: MMR(V) vaccine (live, attenuated).



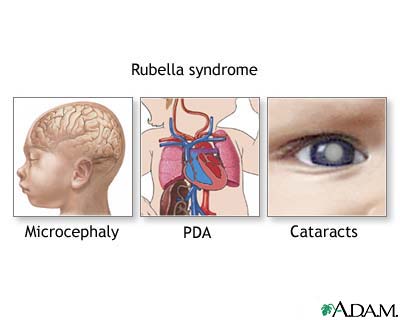
Rubella (German Measles)
Rubella is a mild, contagious disease caused by a single-stranded, positive-sense RNA virus (family Togaviridae). Transmission is via respiratory droplets or vertically across the placenta.
Symptoms: Fever, pale pink maculopapular rash, lymphadenopathy.
Congenital Rubella Syndrome: Infection during pregnancy can cause microcephaly, cataracts, and patent ductus arteriosus (PDA) in the fetus.
Diagnosis: Detection of rubella-specific IgM antibodies.
Treatment: Supportive; no antiviral drugs.
Prevention: MMR(V) vaccine; contraindicated in pregnancy.
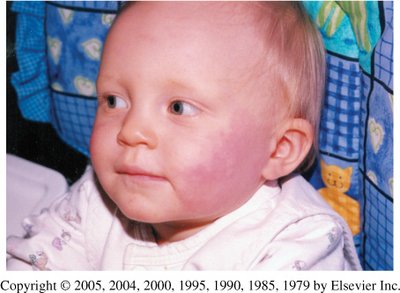
Parvovirus B19 (Erythema Infectiosum, Fifth Disease)
Parvovirus B19 is a non-enveloped, single-stranded DNA virus. It infects red blood cell precursors via the P antigen and is transmitted by the respiratory route.
Symptoms: Fever, coryza, headache, GI distress, "slapped cheek" rash, possible lacy rash on limbs.
Complications: Aplastic crisis in patients with hemolytic anemia.
Diagnosis: Detection of viral nucleic acid, antibody, or antigen.
Treatment: Supportive; immunoglobulin for immunocompromised patients.
Prevention: No vaccine available.
Roseola Infantum (Exanthem Subitum, Sixth Disease)
Roseola is caused primarily by human herpesvirus 6 or 7. It affects children 6 months to 4 years old and is characterized by a sudden high fever followed by a faint rash as the fever subsides.
Symptoms: High fever, possible convulsions, leukopenia, faint maculopapular rash.
Diagnosis: Clinical presentation.
Treatment: Supportive; no vaccine available.

Varicella-Zoster Virus (Chickenpox and Shingles)
Varicella-zoster virus (VZV) is a double-stranded DNA virus in the Herpesviridae family. It causes chickenpox (varicella) in children and can reactivate later in life as shingles (zoster).
Transmission: Respiratory droplets, direct contact with lesions.
Chickenpox: Vesicular rash, fever, highly contagious, virus remains latent in neurons.
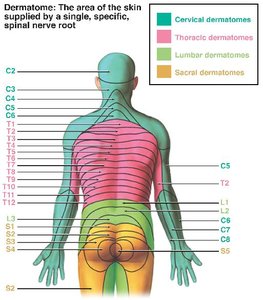
Shingles: Reactivation along a dermatome, painful vesicular rash, postherpetic neuralgia.
Diagnosis: Clinical appearance; shingles lesions do not cross the midline.
Treatment: Acyclovir for shingles; no aspirin for children (risk of Reye's syndrome).
Prevention: Varivax (children), Zostavax (adults >60), both live, attenuated vaccines.


Smallpox (Variola)
Smallpox is a highly contagious disease caused by the variola virus (a poxvirus). Transmission is via respiratory droplets or direct contact with contaminated materials.
Symptoms: Fever, malaise, headache, centrifugal rash (face, arms, legs), lesions develop synchronously.
Progression: Flat red lesions → pus-filled vesicles → crusts → scabs fall off by week 3.
Diagnosis: Clinical presentation, epidemiological context.
Treatment: No antiviral drugs; vaccine can be given post-exposure.
Prevention: Live vaccinia virus vaccine; global eradication achieved in 1980.
Bacterial Skin Pathogens
Streptococcus pyogenes (Group A Streptococcus, GAS)
Streptococcus pyogenes is a Gram-positive, β-hemolytic coccus arranged in chains. It is a facultative anaerobe and a significant cause of pharyngitis and skin infections.
Virulence Factors: M protein (antiphagocytic), hemolysin, streptokinase, hyaluronidase, erythrogenic toxin (scarlet fever).
Diseases: Strep throat, scarlet fever, rheumatic fever, impetigo, cellulitis, necrotizing fasciitis.
Diagnosis: Throat swab, blood agar, rapid strep test.
Treatment: Penicillin, erythromycin.
Prevention: No vaccine; proper hygiene.
Staphylococcus aureus
Staphylococcus aureus is a Gram-positive, facultative anaerobic coccus that forms grape-like clusters. It is salt-tolerant and survives on skin and environmental surfaces.
Virulence Factors: Coagulase, hyaluronidase, staphylokinase, lipases, β-lactamase, cytolytic toxins, exfoliative toxins, toxic shock syndrome toxin, enterotoxins.
Diseases: Food poisoning, skin infections (boils, impetigo, scalded skin syndrome), toxic shock syndrome.
Diagnosis: Catalase-positive, coagulase-positive, mannitol fermenting, β-hemolytic on blood agar.
Treatment: Trimethoprim, doxycycline, IV vancomycin for severe cases.
Prevention: Hand hygiene, infection control in healthcare settings.
Clostridium perfringens
Clostridium perfringens is an anaerobic, Gram-positive, endospore-forming rod. It is found in soil and the intestines of animals.
Virulence Factors: α-toxin (phospholipase C), other toxins and enzymes causing tissue damage.
Diseases: Gas gangrene, cellulitis, foodborne disease.
Diagnosis: Clinical observation, bacteriologic studies.
Treatment: Debridement, penicillin, hyperbaric oxygen therapy.
Prevention: Wound care, hygiene.
Clinical Case Studies
Case 1: Varicella Transmission
Scenario: Child develops chickenpox after visiting a relative with shingles.
Explanation: Shingles lesions shed varicella-zoster virus, which can cause chickenpox in susceptible individuals.
Therapy: Supportive care; Varivax vaccine for prevention.
Case 2: Erythema Infectiosum
Scenario: 8-year-old with fever, malaise, and bright red cheek rash.
Diagnosis: Parvovirus B19 infection (fifth disease).
Therapy: Supportive care; immunoglobulin for immunocompromised.
Case 3 & 4: Cellulitis and Abscess
Scenario: Adult with cellulitis following an ingrown hair; culture reveals catalase and coagulase positive organism (S. aureus).
Antibiotic Resistance: Resistance to cephalexin and penicillin G; susceptible to trimethoprim-sulfamethoxazole, doxycycline, vancomycin.
Therapy: Use antibiotics to which the isolate is susceptible (e.g., trimethoprim-sulfamethoxazole, doxycycline, vancomycin for severe cases).
Summary Table: Exanthems and Enanthems
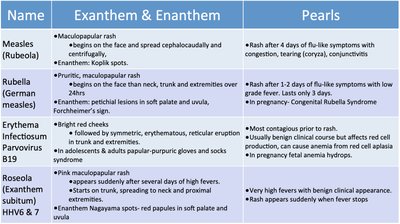
Name | Exanthem & Enanthem | Pearls |
|---|---|---|
Measles (Rubeola) | Maculopapular rash, Koplik spots | Rash after 4 days of prodrome; highly contagious |
Rubella | Pale pink maculopapular rash, Forchheimer spots | Congenital syndrome risk in pregnancy |
Erythema Infectiosum (Parvovirus B19) | Bright red cheeks, lacy rash | Risk of aplastic crisis in hemolytic anemia |
Roseola (HHV-6/7) | Faint maculopapular rash after high fever | Rash appears as fever resolves |
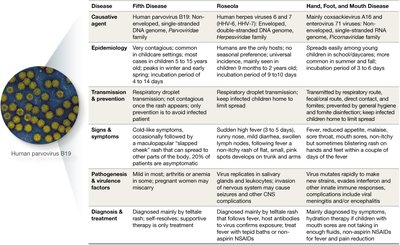
Summary Table: Fifth Disease, Roseola, Hand, Foot, and Mouth Disease
Disease | Causative Agent | Epidemiology | Transmission & Prevention | Signs & Symptoms | Diagnosis & Treatment |
|---|---|---|---|---|---|
Fifth Disease | Parvovirus B19 | Common in children | Respiratory droplets | Slapped cheek rash | Clinical; supportive |
Roseola | HHV-6/7 | Infants, young children | Respiratory droplets | High fever, rash | Clinical; supportive |
Hand, Foot, and Mouth Disease | Coxsackievirus A16 | Young children | Respiratory, fecal-oral | Vesicular rash on hands, feet, mouth | Clinical; supportive |
Additional info: These notes integrate and expand upon the provided material, ensuring coverage of all major pathogens, syndromes, and clinical management strategies relevant to microbiology students studying skin infections.
