 Back
BackMicrobiology of Skin Infections
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Skin Structure and Defenses
Overview of Skin Anatomy
The skin is the largest organ of the human body and serves as a primary barrier against infectious agents. It is composed of multiple layers, each with specialized structures and functions that contribute to its protective role.
Epidermis: The outermost layer, consisting of tightly packed dead cells and living keratinocytes, which produce keratin for waterproofing.
Dermis: A thicker, underlying layer made of connective tissue, blood vessels, nerves, hair follicles, sweat glands, and sebaceous glands.
Subcutaneous Layer: Located beneath the dermis, composed of fat cells, nerves, and blood vessels; not technically part of the skin but closely associated with it.
Skin Defense Mechanisms
The skin employs several defense mechanisms to prevent microbial invasion:
Physical Barrier: Intact epidermis prevents entry of microbes.
Melanin: Provides antimicrobial properties and protects against UV damage.
Perspiration: Acidic pH and high salt content act as chemical barriers; sweat washes away microbes (mechanical barrier).
Lysozyme: Enzyme in sweat that breaks down bacterial peptidoglycans.
Sebum: Oily secretion from sebaceous glands containing low pH lipids and proteins that moisturize and protect the skin.
Skin Microbiome
The skin hosts a diverse community of normal microbiota, which reside in the epidermis, sweat glands, sebaceous glands, and hair follicles. The composition of the skin microbiome is influenced by environmental exposure, occupation, antibiotic use, age, cosmetics, hygiene products, clothing, and hormone levels.
Major Bacterial Phyla: Actinobacteria, Bacteroidetes, Proteobacteria
Common Genera: Staphylococcus, Malassezia (fungus), Pseudomonas, Janthinobacterium
Skin Lesions and Rashes
Definitions and Clinical Importance
Understanding skin lesions and rashes is essential for diagnosing infectious and noninfectious skin diseases. Dermatologists classify lesions as primary (directly associated with a disease process) or secondary (arising from primary lesions or other causes such as scratching or allergic reactions).
Lesion: Any observable abnormality of the skin in a localized area.
Rash: Widespread eruption of lesions, which may be symptomatic or asymptomatic.
Primary Lesions
Vesicle: Small, elevated lesion filled with clear fluid (e.g., chickenpox).
Bulla: Large vesicle (>0.5 cm in diameter; e.g., blister).
Macule: Flat, discolored area (e.g., freckles).
Papule: Raised, solid lesion, not fluid-filled, <0.5 cm (e.g., warts).
Pustule: Raised lesion with pus (e.g., inflammatory acne).
Cyst: Closed, fluid-filled sac, deeper in the skin (e.g., nodular cystic acne).
Maculopapular Rash: Slightly raised papules overlaying or interspersed with macules (e.g., rubella, measles).
Secondary Lesions
Crust: Dried exudate on the skin (e.g., honey-colored crust in impetigo).
Scale: Flaking of outer epidermal layers (e.g., athlete’s foot, psoriasis).
Purpura: Large purple spots from subcutaneous bleeding (3–10 mm; e.g., meningococcal meningitis).
Petechiae: Small pinpoint spots (<3 mm) from capillary bursts (e.g., scarlet fever, drug reactions).
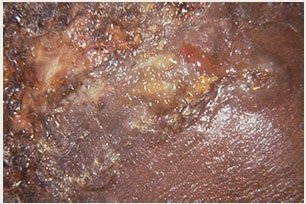
Ulcer: Open sore with destruction of epidermal and dermal layers (e.g., cutaneous anthrax).

Viral Skin Infections
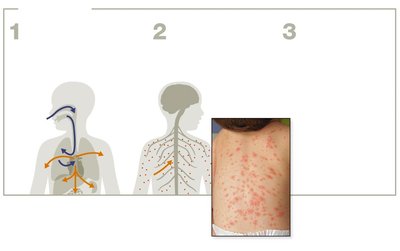
Chickenpox and Shingles
Chickenpox and shingles are caused by the Varicella-zoster virus (Herpesviridae family). Chickenpox is highly contagious and spreads via respiratory droplets and direct contact with lesions. After initial infection, the virus can become latent in peripheral nerves and reactivate later in life as shingles.
Chickenpox: Fever and itchy vesicular rash; more severe in adults.
Shingles: Reactivation of latent virus, causing a painful, banded rash.
Prevention: Live-attenuated varicella vaccine (since 1995); Shingrix vaccine for shingles (protein-based, recommended for adults over 50).
Herpes Simplex Viruses (HSV-1 and HSV-2)
Human herpes simplex viruses 1 and 2 cause vesicular skin lesions. HSV-1 is primarily associated with oral herpes (cold sores), while HSV-2 is more often linked to genital herpes. The viruses can become latent in nerve cells and reactivate due to triggers such as stress or UV exposure.
Transmission: Saliva, contaminated fomites, direct contact.
Diagnosis: Clinical signs, syncytia formation in tissues, PCR analysis.
Treatment: No cure; antivirals reduce severity and frequency of outbreaks.
Maculopapular Viral Rashes
Several viral infections cause maculopapular rashes, including measles (rubeola), rubella, fifth disease, and hand, foot, and mouth disease. These rashes are characterized by small, slightly raised papules overlaying or interspersed with macules.
Measles: Highly contagious, spreads via respiratory route, causes fever, cough, Koplik’s spots, and a characteristic rash.
Complications: Encephalitis, pneumonia, secondary infections, and death in severe cases.
Prevention: MMR vaccine (measles, mumps, rubella).
Warts (Papillomavirus Infections)
Warts are caused by various papillomaviruses and are common, benign skin growths. They are spread by direct contact, contaminated surfaces, or autoinoculation. Types include plantar warts (feet), seed warts (fingers), and flat warts (rest of the body).
Transmission: Direct contact, fomites, autoinoculation.
Clinical Features: Small, rough, thickened skin growths.

Bacterial Skin Infections
Acne Vulgaris
Acne is a common skin condition, especially among adolescents, primarily caused by Propionibacterium acnes. It results from clogged hair follicles and pores, leading to different types of lesions: comedonal (non-inflammatory), inflammatory, and nodular cystic (severe).
Etiology: P. acnes (Gram-positive rods), normal skin residents.
Pathogenesis: Proliferate in clogged pores, degrade sebum, trigger inflammation.
Treatment: Retinoids, antibiotics, laser, phototherapy.
Staphylococcus aureus Skin Infections
Staphylococcus aureus is a leading cause of various skin infections, including impetigo, erysipelas, cellulitis, and scalded skin syndrome. It possesses numerous virulence factors such as coagulase, catalase, hemolysins, and exfoliative toxins.
Impetigo: Superficial, pus-filled vesicles that rupture and form honey-colored crusts; highly contagious.
Erysipelas: Acute infection of the upper dermis and superficial lymphatics; causes fever, chills, and extensive inflammation.
Cellulitis: Infection of the lower dermis and subcutaneous fat; presents as red, swollen, painful skin, often on the legs.
Scalded Skin Syndrome: Exfoliative toxins cause the epidermis to peel in sheets, resembling burns.
Necrotizing Fasciitis (Streptococcus pyogenes)
Necrotizing fasciitis, or "flesh-eating disease," is a rapidly progressing infection caused by Streptococcus pyogenes (Group A Streptococcus). The bacteria produce enzymes and toxins that degrade connective tissues, leading to severe tissue destruction.
Virulence Factors: Hyaluronidase, streptolysins, pyrogenic toxins.
Clinical Features: Rapidly spreading infection, high mortality if untreated.
Pseudomonas aeruginosa Infections
Pseudomonas aeruginosa is a Gram-negative rod that causes opportunistic infections, especially in burn and wound patients. It is notable for its resistance to antibiotics and ability to form biofilms.
Clinical Features: Wound infections, blue-green pus (pyocyanin pigment), tissue damage.
Treatment: Meticulous wound care, antibiotics, silver-containing creams, debridement.
Fungal and Parasitic Skin Infections
Cutaneous Mycoses
Fungal skin infections are usually superficial and caused by dermatophytes or Candida species. Immunocompromised individuals are at higher risk for deeper infections.
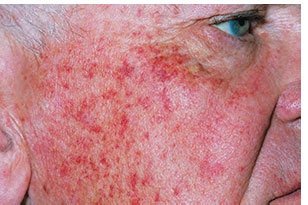
Cutaneous Candidiasis: Caused by Candida albicans; presents as bright red macular rash in damp, friction-prone areas.
Treatment: Keep area dry, topical antifungal creams.
Tinea Infections (Ringworm)
Tinea infections are caused by dermatophytes such as Trichophyton, Microsporum, and Epidermophyton. They affect skin, hair, and nails, leading to scaly, discolored, or inflamed lesions.
Types: Tinea pedis (athlete’s foot), tinea cruris (jock itch), tinea capitis (scalp), tinea unguium (nails), tinea corporis (body).
Treatment: Topical or oral antifungals (e.g., terbinafine, griseofulvin).
Cutaneous Leishmaniasis
Leishmaniasis is a protozoan infection transmitted by the bite of infected sand flies. It is prevalent in tropical and subtropical regions.
Cutaneous Form: Painless skin ulcers at bite sites, can persist for months or years, may cause scarring.
Mucocutaneous Form: Lesions in mucous membranes, leading to severe disfigurement.
Visceral Form: Systemic spread, fatal if untreated.
Prevention: Avoid sand fly bites, use insect repellents, cover exposed skin.
Treatment: Sodium stibogluconate, amphotericin B, miltefosine.
