 Back
BackPathogenic Fungi: Systemic and Opportunistic Mycoses
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Pathogenic Fungi
Overview of Systemic Mycoses
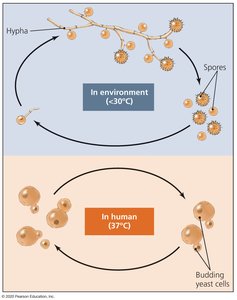
Systemic mycoses are fungal infections that affect internal organs and are often acquired through inhalation. Four major genera—Histoplasma, Blastomyces, Coccidioides, and Paracoccidioides—are responsible for these diseases. All are dimorphic fungi, meaning they grow as mycelial thalli in the environment and as spherical yeasts in the human body.
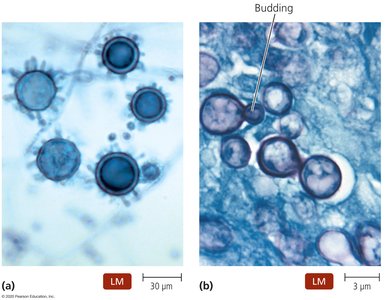
Dimorphism: Environmental form (hyphae and spores) vs. human form (budding yeast cells).
Transmission: Inhalation of spores is the primary route.
Pathogenesis: Begins as pulmonary infection, can disseminate via blood.
Histoplasmosis
Histoplasma capsulatum is the most common fungal pathogen affecting humans. It thrives in moist soils with high nitrogen content and is acquired mainly by inhaling spores. Once in the lungs, the fungus is phagocytized by macrophages and can spread via blood and lymph.
Clinical Manifestations: Usually asymptomatic; four main disease types: chronic pulmonary, chronic cutaneous, systemic, and ocular histoplasmosis.
Diagnosis: Identification of yeast in patient samples.
Treatment: Amphotericin B or ketoconazole for severe cases.


Blastomycosis
Blastomyces dermatitidis causes blastomycosis, found in soils rich in organic matter. Pulmonary blastomycosis is the most common manifestation, often asymptomatic but can become chronic. The fungus can also cause cutaneous, osteoarticular, and CNS infections.
Diagnosis: Identification of fungi in culture or samples.
Treatment: Oral itraconazole or amphotericin B; relapse common in AIDS patients.

Coccidioidomycosis (Valley Fever)
Coccidioides immitis is found in desert soils of the southwestern US and northern Mexico. Infection rates have risen due to population expansion and increased recreational activities. Inhaled arthroconidia germinate into spherules in the lung, releasing spores.
Clinical Manifestations: Pulmonary conditions, often asymptomatic; serious infections in immunocompromised individuals.
Diagnosis: Presence of spherules in patient samples or positive skin test.
Treatment: Amphotericin B; maintenance therapy for AIDS patients.


Paracoccidioidomycosis
Paracoccidioides brasiliensis is found in southern Mexico and South America, mainly affecting farm workers. The infection begins as a pulmonary condition and can spread to create lesions. Diagnosis is based on the presence of yeast in a "steering wheel" formation.
Treatment: Itraconazole, ketoconazole, or amphotericin B.

Opportunistic Fungal Pathogens
Overview
Opportunistic mycoses primarily affect individuals with compromised immunity or disrupted microbiomes. The five most common opportunists are Pneumocystis, Candida, Aspergillus, Cryptococcus, and Mucor.
Risk Factors: AIDS, cancer, diabetes, immunosuppressive therapy.
Diagnosis: Often challenging due to atypical symptoms.
Pneumocystis Pneumonia
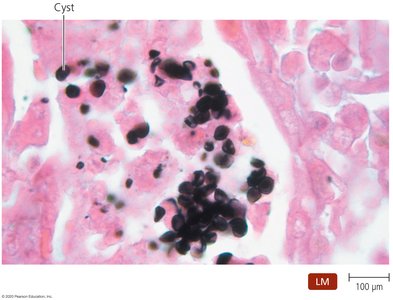
Pneumocystis jirovecii is a common opportunistic infection in AIDS patients, almost diagnostic for AIDS. Transmission is likely via inhalation, and most people are exposed by age five. Infection in immunocompetent individuals is usually asymptomatic.
Diagnosis: Clinical and microscopic findings.
Treatment: Trimethoprim and sulfamethoxazole.
Aspergillosis
Diseases caused by Aspergillus species result from inhalation of spores. Three clinical pulmonary diseases may develop: hypersensitivity (asthma/allergy), noninvasive (fungal masses in lung cavities), and acute invasive (pneumonia).
Diagnosis: Clinical history, abnormal lung structure, identification of septate hyphae and conidia in samples.
Treatment: Allergy medications for hypersensitivity; surgical removal and intravenous voriconazole for invasive disease; itraconazole for maintenance in AIDS patients.


Cryptococcosis
Cryptococcus neoformans causes cryptococcosis, with two varieties: C. neoformans gattii (immunocompetent) and C. neoformans neoformans (AIDS patients). Infection results from inhalation of spores or dried yeast in bird droppings. The fungus resists phagocytosis and has a predilection for the CNS.
Clinical Manifestations: Pulmonary, meningitis, cryptococcoma, cutaneous forms.
Diagnosis: Identification of fungus in patient samples.
Treatment: Amphotericin B and 5-fluorocytosine; fluconazole for maintenance.

Mucormycosis and Microsporidiosis
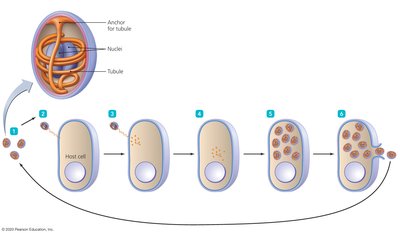
Mucormycosis is caused by Mucor species, common in the environment. Infections develop in the face and head, especially in diabetics, cancer patients, and drug users. Microsporidiosis is caused by obligate intracellular fungi, including Microsporidium, Encephalitozoon, and Nosema.
Mucormycosis: Can cause rhinocerebral, pulmonary, gastrointestinal, cutaneous infections. Diagnosis is by microscopy; treatment is removal of infected tissue and amphotericin B.
Microsporidiosis: Primarily affects immunocompromised; severe diarrhea is common. Diagnosed by microscopy, TEM, immunoassays, PCR; treated with albendazole.
Fungal Pathogens in Covid-19 Patients
Opportunistic Fungi in Covid-19
Patients with severe Covid-19 are vulnerable to opportunistic fungal infections, especially pulmonary aspergillosis and invasive candidiasis. Early diagnosis and treatment are critical.
Diagnosis: CAPA involves lower respiratory tract specimens and testing for Aspergillus galactomannan antigen; candidemia diagnosed by symptoms and fungal culture.
Treatment: Early intervention is essential.
Clinical Manifestations of Candidiasis
Table: Types, Symptoms, and Predisposing Factors
Candidiasis presents in various forms, each with distinct clinical signs and predisposing factors. The following table summarizes these manifestations:
Type | Clinical Signs and Symptoms | Predisposing Factors |
|---|---|---|
Oropharyngeal (thrush) | White plaques on mouth, tongue, gums, palate, pharynx | Diabetes, AIDS, cancers, chemotherapy |
Cutaneous | Moist red rash between skin folds, diaper rash, onychomycosis | Moisture, heat, friction, obesity, immunocompromised |
Vulvovaginal | Creamy discharge, burning, redness, painful intercourse | Antibiotics, pregnancy, diabetes, microbiome changes |
Chronic mucocutaneous | Lesions on skin, nails, mucous membranes | Impaired cell-mediated immunity |
Neonatal and congenital | Meningitis, renal disorders, generalized rash | Young age, low birth weight, maternal antibiotics |
Esophageal | White plaques, burning pain, nausea, vomiting | AIDS, immunocompromised |
Gastrointestinal | Ulceration of stomach and intestinal mucosa | Hematological cancers |
Pulmonary | Nonspecific symptoms, often undiagnosed | Spread from other candidiasis types |
Peritoneal | Fever, pain, tenderness | Dialysis catheters, GI perforation |
Urinary tract | Painful urination, discharge | Catheterization, diabetes, bladder problems |
Meningeal | Swelling, fever, headache, neck stiffness | Systemic spread |
Renal | Fever, pain, fungus ball | Additional info: Often associated with systemic infection |
Hepatic and splenic | Fever, swelling, dysfunction, lesions | Leukemia |
Endocardial, myocardial, pericardial | Fever, murmur, heart failure, anemia | Valve disease, catheterization, IV drug abuse |
Ocular | Cloudy vision, eye lesions | Spread, catheters, IV drug abuse, trauma |
Osteoarticular | Pain on weight-bearing | Spread, prosthetic implants |
Candidemia | Antibiotic-resistant fever, tachycardia, hypotension, skin lesions, organ abscesses | Catheters, antibacterial drugs, surgery, burns |
Laboratory Diagnosis and Media
Preferred Media for Fungal Culture
Saroubaud dextrose agar is the preferred medium for culturing fungi due to its ability to support fungal growth while inhibiting bacterial contamination.
Techniques for Detecting Fungal Cells in Tissues
Both KOH preparation and GMS staining are effective techniques for revealing the presence of fungal cells in tissues. KOH dissolves host tissue, making fungal elements more visible, while GMS stains fungal cell walls.
Summary
This guide covers the major systemic and opportunistic fungal pathogens, their clinical manifestations, diagnosis, treatment, and laboratory techniques. Understanding these concepts is essential for recognizing and managing fungal diseases in clinical practice.
