 Back
BackPathogenic Gram-Positive Bacteria: Structure, Diseases, and Clinical Management
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Pathogenic Gram-Positive Bacteria
Overview
Gram-positive bacteria are a diverse group of microorganisms that can cause a variety of diseases in humans. This section focuses on clinically significant genera, including Bacillus, Clostridium, Listeria, and Mycoplasma. These bacteria are characterized by their thick peptidoglycan cell walls and, in some cases, their ability to form endospores, which contribute to their resilience and pathogenicity.
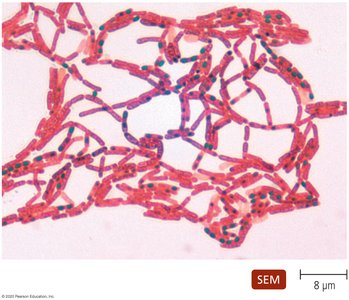
Bacillus
Structure and Physiology
Endospore formation: Bacillus species can form highly resistant endospores, allowing survival in harsh environments.
Cell morphology: Bacilli occur singly, in pairs, or in chains.
Oxygen requirements: Most are facultative anaerobes.
Pathogenicity: Bacillus anthracis is the primary human pathogen, causing anthrax.
Epidemiology and Transmission
Humans contract anthrax from infected animals or animal products.
Transmission routes include inhalation, inoculation through skin breaks, and ingestion of spores.
Diseases Caused by Bacillus anthracis
Gastrointestinal anthrax: Rare in humans; results from ingestion of spores.
Inhalation anthrax: Rare but highly lethal; requires inhalation of airborne endospores.
Cutaneous anthrax: Most common; produces a characteristic ulcer called an eschar. Untreated, it is fatal in about 20% of cases.

Diagnosis, Treatment, and Prevention
Diagnosis: Identification of large, non-motile, Gram-positive bacilli in clinical samples.
Treatment: Many antimicrobials are effective (e.g., ciprofloxacin, doxycycline).
Prevention: Control in animals and vaccination (requires multiple doses and boosters).
Clostridium
Structure and Physiology
Endospore formation: All clinically important species form endospores.
Oxygen requirements: Obligate anaerobes.
Habitat: Ubiquitous in soil, water, and the gastrointestinal tracts of animals and humans.
Common pathogens: C. difficile, C. botulinum, C. tetani, C. perfringens.

Clostridium difficile
Pathogenesis, Epidemiology, and Disease
Common intestinal microbiota; opportunistic in patients on broad-spectrum antibiotics.
Produces toxins A and B, and hyaluronidase.
Minor infections: Self-limiting diarrhea.
Severe cases: Pseudomembranous colitis—sections of colon wall slough off, leading to life-threatening infection.
Diagnosis, Treatment, and Prevention
Diagnosis: Isolation from feces; detection of toxins by immunoassay.
Treatment: Discontinue causative antibiotic; severe cases require targeted antibiotics (e.g., vancomycin).
Prevention: Proper hygiene to limit nosocomial spread.
Clostridium botulinum
Pathogenesis
Produces seven distinct botulinum toxins—among the most potent known.
Toxins bind neurons, preventing acetylcholine release and muscle contraction (flaccid paralysis).
Epidemiology and Disease
Foodborne botulism: Ingestion of preformed toxin; can cause asphyxiation.
Pediatric (infant) botulism: Ingestion of spores; rare paralysis and death.
Wound botulism: Contamination of wounds; symptoms similar to foodborne botulism.
Diagnosis, Treatment, and Prevention
Diagnosis: Based on clinical symptoms.
Treatment: Gastric lavage, antitoxin administration, and antibiotics for wound/infant cases.
Prevention: Proper canning of food; infants under one year should not consume honey.
Clostridium tetani
Structure and Physiology
Motile, obligate anaerobic bacilli with terminal endospores.
Common in soil, dust, and GI tracts.
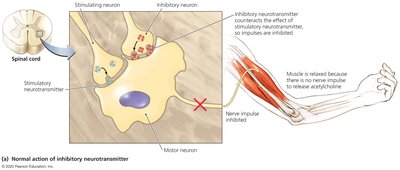
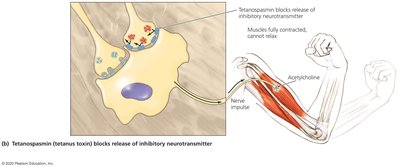
Pathogenesis
Produces tetanospasmin (tetanus toxin), a potent neurotoxin.
Toxin blocks inhibitory neurotransmitter release, causing continuous muscle contraction (spastic paralysis).
Epidemiology and Disease
Initial symptoms: Jaw and neck muscle tightening ("lockjaw").
Progresses to generalized muscle spasms; diaphragm involvement can be fatal.
High mortality rate, especially in areas with poor vaccination coverage.

Diagnosis, Treatment, and Prevention
Diagnosis: Based on characteristic muscle contractions.
Treatment: Wound debridement, antitoxin (immunoglobulin), antibiotics, and supportive care.
Prevention: Immunization with tetanus toxoid (DTaP vaccine).
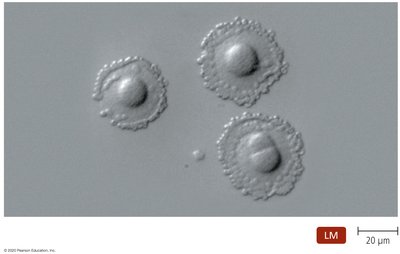
Clostridium perfringens
Overview and Diseases
Large, non-motile, endospore-forming bacillus.
Most frequently isolated Clostridium from clinical specimens.
Causes food poisoning (mild, self-limited) and gas gangrene (severe, tissue necrosis).

Diagnosis, Treatment, and Prevention
Diagnosis: Detection in food/feces; clinical appearance of gas gangrene.
Treatment: Food poisoning is self-limited; gas gangrene requires surgical removal of dead tissue, antitoxin, and penicillin.
Prevention: Refrigeration of foods; proper wound care.
Listeria
Structure and Physiology
Non-endospore-forming, Gram-positive rod.
Found in soil, water, and animals; enters via contaminated food/drink.
Pathogenesis, Epidemiology, and Disease
Listeria monocytogenes is an intracellular pathogen, growing in phagocytes (often in the gall bladder).
Virulence is linked to its ability to survive within cells, aided by listeriolysin O.
Can cause meningitis, especially in neonates, pregnant women, elderly, and immunocompromised.
Pregnant women can transmit infection to the fetus, causing miscarriage, stillbirth, or neonatal meningitis.
Diagnosis, Treatment, and Prevention
Diagnosis: Isolation from cerebrospinal fluid; rarely seen in Gram stains.
Treatment: Ampicillin is the drug of choice; alternatives for penicillin-allergic patients.
Prevention: At-risk individuals should avoid high-risk foods (e.g., unpasteurized dairy, deli meats).
Mycoplasmas
Structure and Physiology
Smallest free-living microbes; lack cell walls and have sterols in their membranes.
Require complex growth factors; colonize mucous membranes of respiratory and urinary tracts.
Associated with pneumonia and urinary tract infections.
Pathogenesis, Epidemiology, and Disease
Mycoplasma pneumoniae attaches to respiratory epithelium, impairing mucus removal.
Causes primary atypical pneumonia ("walking pneumonia"); symptoms are mild and often do not require hospitalization.
Common in children 5–15 years old; spread by nasal secretions.
Diagnosis, Treatment, and Prevention
Diagnosis: Difficult due to small size and slow growth; culture and serology may be used.
Treatment: Macrolides, doxycycline, or fluoroquinolones.
Prevention: Good hygiene and avoidance of aerosols/fomites; asymptomatic carriers are common.
Other Mycoplasmas
M. hominis, M. genitalium, and Ureaplasma urealyticum are associated with urogenital infections.
Can cause nongonococcal urethritis and pelvic inflammatory disease (PID).
Treatment: Various antibiotics; prevention includes safe sex practices.
Review Questions
Which Clostridium species causes pseudomembranous colitis after broad-spectrum antibiotic use? Answer: Clostridium difficile
Most Bacillus species are facultative anaerobes; Clostridium species are: Answer: Anaerobes
Tetanospasmin acts on neurons in the _____ to block muscle relaxation: Answer: Central nervous system
