 Back
BackPathogenic Gram-Positive Cocci: Staphylococcus, Streptococcus, and Enterococcus
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Pathogenic Gram-Positive Bacteria
Introduction
This section covers the structure, physiology, pathogenicity, epidemiology, diseases, diagnosis, treatment, and prevention of major Gram-positive cocci, focusing on Staphylococcus, Streptococcus, and Enterococcus. These bacteria are significant human pathogens responsible for a wide range of diseases, from mild skin infections to life-threatening systemic illnesses.
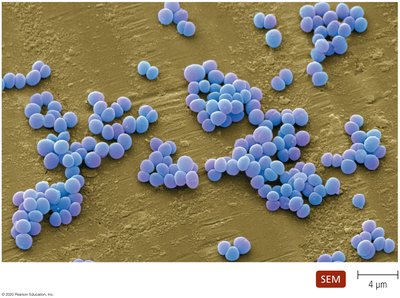
Staphylococcus: Structure, Physiology, and Pathogenicity
Structure and Physiology
Cell Arrangement: Cells occur in grape-like clusters.
Motility: Non-motile.
Oxygen Requirements: Facultative anaerobes.
Catalase: Catalase-positive (distinguishes from Streptococcus).
Antibiotic Resistance: Most are resistant to Penicillin G.
Salt Tolerance: Can tolerate high salt concentrations, allowing survival on human skin.
Environmental Resistance: Tolerant of desiccation, radiation, and heat; survive on environmental surfaces.
Medically Important Species
Staphylococcus aureus: More virulent; causes a variety of diseases depending on infection site; coagulase positive.
Staphylococcus epidermidis: Part of normal skin microbiota; causes opportunistic infections, especially in immunocompromised hosts or with indwelling devices.
Pathogenicity Mechanisms
Staphylococcal infections occur when bacteria breach the body's physical barriers. Pathogenicity is due to:
Structural defenses against phagocytosis:
Slime layers (capsules): Inhibit leukocyte chemotaxis and phagocytosis; facilitate attachment to surfaces.
Protein A (S. aureus): Binds IgG, inhibiting opsonization and complement activation.
Bound coagulase (S. aureus): Converts fibrinogen to fibrin, forming clots that hide bacteria from immune cells.
Enzymes:
Cell-free coagulase (S. aureus): Triggers blood clotting.
Hyaluronidase (S. aureus): Breaks down hyaluronic acid, aiding tissue invasion.
Staphylokinase (S. aureus): Dissolves fibrin clots, allowing bacterial spread.
Lipases (S. aureus & S. epidermidis): Digest lipids, enabling growth on skin and in oil glands.
Beta-lactamase (S. aureus): Breaks down penicillin, conferring antibiotic resistance.
Toxins (mainly S. aureus):
Cytolytic toxins: Disrupt cell membranes; leukocidin lyses leukocytes.
Exfoliative toxins: Cause skin cells to separate and slough off.
Toxic-shock syndrome toxin (TSST-1): Causes systemic effects.
Enterotoxins: Cause food poisoning symptoms.
Virulence Factor Comparison Table
Virulence Factor | S. aureus | S. epidermidis |
|---|---|---|
Protein A | + | − |
Coagulase | + | − |
Slime layer | + | + |
Catalase | + | + |
Hyaluronidase | + | − |
Staphylokinase | + | − |
Lipase | + | + |
β-lactamase | + | − |
Toxins | + | − |
Epidemiology
S. epidermidis: Ubiquitous on human skin.
S. aureus: Primarily found on moist skin folds.
Both species can colonize the upper respiratory, gastrointestinal, and urogenital tracts.
Transmission occurs via direct contact and fomites.
Handwashing and aseptic techniques are critical for prevention.
Staphylococcal Diseases
Exotoxin-mediated diseases (S. aureus):
Gastroenteritis (food poisoning): Non-invasive; caused by ingestion of enterotoxin-contaminated food.
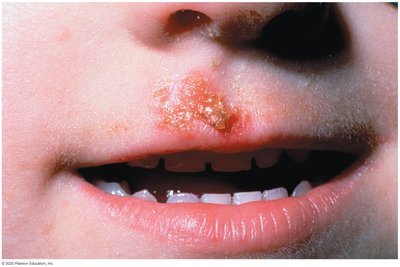
Scalded Skin Syndrome: Cutaneous disease caused by exfoliative toxin.
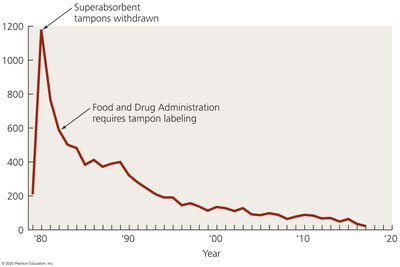
Toxic Shock Syndrome (TSS): Systemic disease caused by TSST-1.
Direct organ invasion:
Bacteremia: Bacteria in the blood.
Endocarditis: Infection of the heart lining.
Pneumonia and empyema: Lung infections.
Osteomyelitis: Infection of bone and bone marrow.
Cutaneous infections: Impetigo, folliculitis.


Diagnosis, Treatment, and Prevention
Diagnosis: Gram-positive cocci in clusters; coagulase test for S. aureus.
Treatment: Methicillin; vancomycin for MRSA (methicillin-resistant S. aureus).
Prevention: Hand antisepsis is crucial, especially in healthcare settings.
Streptococcus: Structure, Physiology, and Pathogenicity
Structure and Physiology
Cell Arrangement: Cocci in pairs or chains.
Oxygen Requirements: Facultative anaerobes.
Catalase: Catalase-negative (distinguishes from Staphylococcus).
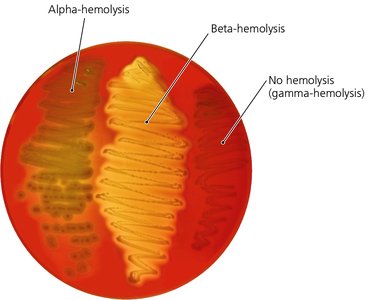
Classification: Based on hemolytic activity (alpha, beta, gamma) and Lancefield grouping (A, B, etc.).
Significant Human Pathogens: Groups A and B.
Group A Streptococcus (Streptococcus pyogenes)
Structural defenses:
M protein: Destabilizes complement, inhibits phagocytosis.
Hyaluronic acid capsule: Camouflages bacteria from immune cells.
Enzymes:
Streptokinases: Break down blood clots, aiding spread.
Deoxyribonucleases: Reduce pus viscosity, facilitating spread.
C5a peptidase: Degrades complement protein C5a, reducing leukocyte recruitment.
Hyaluronidase: Facilitates tissue invasion.
Toxins:
Pyrogenic toxins: Cause fever, rash, and shock.
Streptolysins: Lyse red and white blood cells, and platelets.
Epidemiology
Infects pharynx or skin; disease often follows depletion of normal microbiota.
Spread via respiratory droplets.
Diseases Caused by S. pyogenes
Local invasion/exotoxin release:
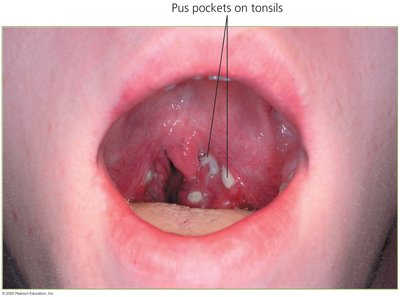
Pharyngitis (strep throat): Inflammation of the pharynx.
Scarlet fever: Rash following pharyngitis, caused by pyrogenic toxin.
Streptococcal TSS: Severe multisystem infection, can cause organ failure and death.
Pyoderma: Pus-producing skin lesion.
Erysipelas: Infection and inflammation of lymph nodes.
Cellulitis: Inflammation of deeper skin layers.
Necrotizing fasciitis: Rapid tissue destruction, high mortality.
Delayed antibody-mediated diseases:
Rheumatic fever: Autoimmune response damaging heart valves and muscle.
Glomerulonephritis: Immune complexes in kidneys cause inflammation, hypertension, and possible irreversible damage.

Diagnosis, Treatment, and Prevention
Diagnosis: Gram-positive cocci in chains/pairs; rapid strep test for respiratory infections.
Treatment: Penicillin is effective.
Prevention: Antibodies against M protein provide protection.
Group B Streptococcus (Streptococcus agalactiae)
Structure: Cocci in chains; distinguished from group A by group-specific antigens and smaller beta-hemolysis zone.
Pathogenicity: Infects newborns lacking specific antibodies; produces enzymes of unclear function.
Epidemiology: Colonizes GI, genital, and urinary tracts; newborns often infected at birth.
Diseases, Diagnosis, and Prevention
Diseases: Neonatal bacteremia, meningitis, pneumonia; also affects immunocompromised adults.
Diagnosis: ELISA test for group B antigen.
Treatment: Penicillin or ampicillin.
Prevention: Prophylactic penicillin during childbirth; immunization of women can protect future children.
Other Beta-Hemolytic Streptococci
Streptococcus equisimilis: Causes pharyngitis.
Streptococcus anginosus: Produces pus-filled abscesses.
Penicillin is effective against both.
Alpha-Hemolytic Streptococci: The Viridans Group
Produce green pigment on blood agar (alpha-hemolysis).
Lack group-specific carbohydrates; not classified by Lancefield system.
Inhabit mouth, pharynx, GI, genital, and urinary tracts.
Opportunistic pathogens: cause abscesses, dental caries, endocarditis, and meningitis if entering the blood.
Streptococcus pneumoniae
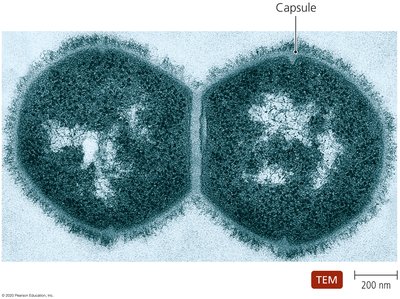
Structure: Diplococci, form unpigmented alpha-hemolytic colonies on blood agar; lack Lancefield antigens.
Pathogenesis and Epidemiology: Present in mouths/pharynx; disease occurs when bacteria reach lungs. Most common in children and elderly.
Diseases: Pneumococcal pneumonia, sinusitis, otitis media, bacteremia, endocarditis, meningitis (high mortality).
Diagnosis, Treatment, and Prevention
Diagnosis: Gram stain of sputum; Quellung reaction confirms capsule.
Treatment: Penicillin (resistant strains exist).
Prevention: Vaccine from purified capsule material.
Enterococcus: Structure, Physiology, and Pathogenicity
Structure and Physiology
Previously classified with group D streptococci; now a separate genus.
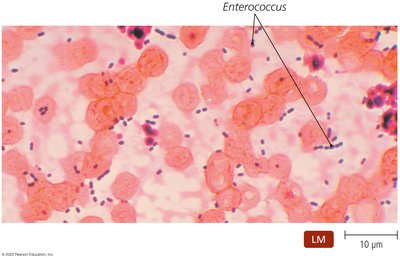
Form short chains and pairs; lack a capsule.
Two main species: Enterococcus faecalis and E. faecium.
All enterococci inhabit the intestinal tracts of animals.
Pathogenesis, Epidemiology, and Disease
Normally found in the human colon; rarely pathogenic there.
Can cause disease if introduced to other body sites (e.g., urinary tract, bloodstream).
Important cause of healthcare-associated infections, especially in immunocompromised patients.
Diagnosis, Treatment, and Prevention
Diagnosis: Distinguished from S. pneumoniae by bile sensitivity.
Treatment: Often resistant to antimicrobials; infections are difficult to treat.
Prevention: Good hygiene and aseptic techniques are essential; prevention is challenging in healthcare settings.
Summary Table: Characteristics of Pathogenic Streptococci
Lancefield Group | Scientific Name | Hemolytic Pattern | Significant Characteristics | Characteristic Diseases |
|---|---|---|---|---|
A | S. pyogenes | Large zone of beta-hemolysis | 1-2 mm white colonies; bacitracin sensitive | Pharyngitis, rheumatic fever, scarlet fever, pyoderma, erysipelas, cellulitis, TSS, necrotizing fasciitis, glomerulonephritis |
B | S. agalactiae | Small zone of beta-hemolysis | 2-3 mm buttery colonies; bacitracin resistant | Puerperal fever, neonatal bacteremia, meningitis, pneumonia |
C | S. equisimilis | Large zone of beta-hemolysis | 1-2 mm white colonies | Pharyngitis, glomerulonephritis |
C, F, or G | S. anginosus | Small zone of beta-hemolysis | 1-2 mm white colonies | Pharyngitis |
— | S. mutans (Viridans group) | Alpha-hemolysis | Green pigment on blood agar | Dental caries, rarely bacteremia, meningitis, endocarditis |
— | S. pneumoniae | Alpha (aerobic), beta (anaerobic) | Diplococci; capsule required for pathogenicity; bile sensitive | Pneumonia, sinusitis, otitis media, bacteremia, endocarditis, meningitis |
D | Enterococcus faecalis, E. faecium | None (gamma-hemolysis) | Diplococci or short chains; no capsule; bile insensitive | UTIs, bacteremia, endocarditis, wound infections |
Key Concepts and Review Questions
Most staphylococci are resistant to penicillin because they express the enzyme: Beta-lactamase.
Streptococcus pyogenes produces ________ which can cause fever, rashes, and shock: Pyrogenic toxins.
Enterococcus can be differentiated from Streptococcus pneumoniae by: Growth in bile.
