 Back
BackPathogenic Microbes and Microbial Infections: Skin, Digestive, and Systemic Diseases
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Clostridium perfringens and Gas Gangrene
Pathogenesis and Clinical Features
Clostridium perfringens is a Gram-positive, anaerobic, endospore-forming bacterium responsible for gas gangrene, a rapidly spreading myonecrosis. Endospores germinate in ischemic tissues, colonizing anaerobic environments and producing toxins that destroy tissue.
Rapidly spreading myonecrosis: Characterized by tissue death and gas production.
Treatment: Surgical debridement of necrotic tissue is essential.
Helicobacter pylori and Gastric Ulcers
Pathogenesis and Clinical Impact
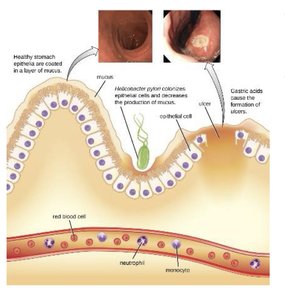
Helicobacter pylori is a helical, acidophilic, Gram-negative bacterium that colonizes the stomach lining, causing ulcers and increasing the risk of stomach cancer. It was discovered in stomach biopsy specimens in 1979 and is responsible for 90% of stomach and duodenal ulcers.
Colonization: H. pylori colonizes the gastric mucosa, decreasing mucus production and exposing epithelial cells to gastric acids.
Ulcer formation: Gastric acids damage the exposed epithelium, leading to ulceration.
Clinical significance: Cofactor in stomach cancer development.
Listeria monocytogenes and Listeriosis
Pathogenesis and Clinical Features
Listeria monocytogenes is a Gram-positive, psychrophilic rod acquired via contaminated foods. It can cause meningitis, especially in neonates and the elderly, and is a leading cause of death from foodborne illness. Listeria can cross the blood-brain barrier and placenta, leading to severe outcomes such as spontaneous abortion.
Growth range: 0°C to 50°C, allowing growth in refrigerated foods.
Dissemination: Capable of spreading through blood and lymph.
Diagnosis: Blood or CSF culture.
Treatment: Antibiotics.
Cellular Invasion Mechanism
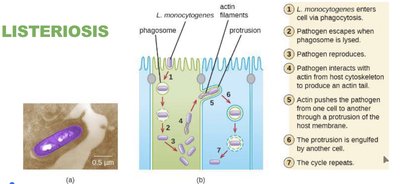
Phagocytosis: Listeria enters host cells via phagocytosis.
Escape: Pathogen escapes from the phagosome and reproduces.
Actin-based motility: Listeria interacts with host actin to produce protrusions, facilitating cell-to-cell spread.
Ebola Virus and Hemorrhagic Fever
Pathogenesis and Epidemiology
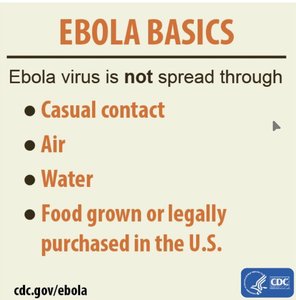
Ebola virus, a member of the Filoviridae family, causes hemorrhagic fever with high mortality rates. The natural reservoir is unknown, but bats are likely hosts. The virus is highly contagious and shed in body fluids, with direct contact being the primary mode of transmission.
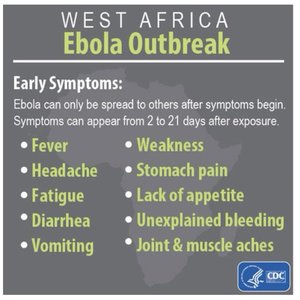
Incubation period: 2–21 days before symptoms appear.
2014 West Africa outbreak: Largest outbreak in history, with 15,261 lab-confirmed cases and 11,325 deaths.
Symptoms: Extensive bleeding, fever, headache, fatigue, diarrhea, vomiting, weakness, stomach pain, lack of appetite, unexplained bleeding, joint and muscle aches.
Streptococcus pyogenes and Skin Infections
Pathogenesis and Clinical Manifestations
Streptococcus pyogenes is a Gram-positive coccus arranged in chains, causing various skin infections once the skin barrier is breached. It is associated with cellulitis, erysipelas, and erythema nodosum.
Cellulitis: Infection of dermis/hypodermis, presenting as a painful, red, warm rash.
Erysipelas: Raised rash with clear borders.
Erythema nodosum: Inflammation of subcutaneous fat cells, leading to red nodules, typically on the lower legs.
Virulence factors: Hyaluronidase, streptokinase, streptolysins, capsule, M proteins.

Necrotizing Fasciitis
Pathogenesis and Clinical Features
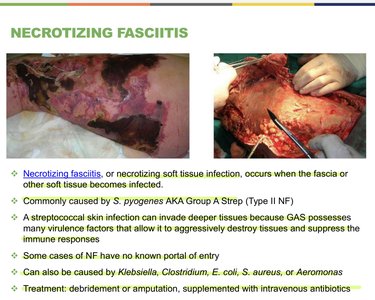
Necrotizing fasciitis is a severe soft tissue infection that occurs when the fascia or other soft tissue becomes infected. It is commonly caused by Streptococcus pyogenes (Type II NF), but can also be caused by Klebsiella, Clostridium, E. coli, S. aureus, or Aeromonas.
Virulence factors: Allow bacteria to destroy tissues and suppress immune responses.
Portal of entry: Some cases have no known entry point.
Treatment: Debridement or amputation, supplemented with intravenous antibiotics.
Pathogenic Strains of Escherichia coli
Enterotoxigenic E. coli (ETEC)
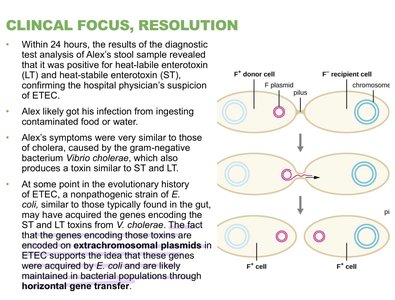
ETEC is a major cause of "traveler’s diarrhea" or Montezuma’s Revenge. It produces heat-stable (ST) and heat-labile (LT) toxins, stimulating secretion and fluid loss. ETEC attaches firmly to the intestinal wall and is usually mild and self-limiting, but elderly and children are at higher risk.
Toxins: ST and LT toxins stimulate chloride ion secretion, leading to water loss and diarrhea.
Virulence factors: Plasmid-encoded toxins.
Enteroinvasive E. coli (EIEC)
EIEC causes inflammatory disease of the large intestine by penetrating epithelial cells, leading to inflammation and tissue damage.
Enteropathogenic E. coli (EPEC)
EPEC is linked to infantile diarrhea, forming pathogenicity islands (pedestals) in the intestine that prevent dislodgement during diarrhea. This can be fatal and is associated with wasting forms of infantile diarrhea.
Enterohemorrhagic E. coli (EHEC/STEC)
EHEC, especially the O157:H7 strain, produces Shiga-toxin (verotoxin) and can cause hemolytic uremic syndrome (HUS), leading to kidney failure. Symptoms range from mild to severe, including bloody diarrhea and HUS.
Shiga-toxin: Inhibits protein synthesis in host cells, causing cell death.
HUS: Characterized by hemolytic anemia, thrombocytopenia, and renal failure.
Summary Table: Pathogenic Microbes and Associated Diseases
Pathogen | Disease | Key Features | Treatment |
|---|---|---|---|
Clostridium perfringens | Gas gangrene | Endospore-forming, anaerobic, rapid myonecrosis | Surgical debridement |
Helicobacter pylori | Gastric ulcers | Acidophile, colonizes stomach, ulcers, cancer risk | Antibiotics, acid suppression |
Listeria monocytogenes | Listeriosis | Psychrophile, crosses BBB/placenta, foodborne | Antibiotics |
Ebola virus | Hemorrhagic fever | Filoviridae, high mortality, body fluid transmission | Supportive care |
Streptococcus pyogenes | Skin infections, necrotizing fasciitis | Gram-positive cocci, virulence factors | Antibiotics, debridement |
ETEC | Traveler’s diarrhea | Heat-stable/labile toxins, mild diarrhea | Supportive care |
EHEC | Bloody diarrhea, HUS | Shiga-toxin, O157:H7, kidney failure | Supportive care, possible antibiotics |
Additional info: Academic context was added to clarify mechanisms, clinical features, and treatment options for each pathogen.
