 Back
BackPathogenic Microorganisms of the Respiratory Tract: Mini-Textbook Study Notes
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Respiratory Tract Anatomy and Defenses
Anatomy of the Respiratory Tract
The respiratory tract is divided into two main sections: the upper and lower respiratory tracts. Each section contains specific anatomical structures that play roles in respiration and defense against pathogens.
Upper respiratory tract: Includes the mouth, nose, nasal cavity, sinuses, throat (pharynx), and epiglottis.
Lower respiratory tract: Comprises the trachea, bronchi, bronchioles, and alveoli.

Defenses of the Respiratory Tract
The respiratory tract employs multiple defense mechanisms to prevent infection by pathogenic microorganisms.
Anatomical defenses: Nasal hair traps particles; cilia propel particles upward and out; mucus traps invading microorganisms.
Immunological defenses: Complement proteins, antimicrobial peptides, chemocytokines, macrophages, and secretory IgA provide additional protection.

Normal Biota of the Respiratory Tract
Composition and Function
The respiratory tract harbors a diverse community of normal biota, which can include bacteria, fungi, and other microorganisms. These biota play a crucial role in microbial antagonism, reducing the chances of pathogenic colonization by competing for resources and space.
Key normal biota: Streptococcus pyogenes, Haemophilus influenzae, Streptococcus pneumoniae, Neisseria meningitidis, Candida albicans.
Microbial antagonism: Example: Lactobacillus sakei suppresses Corynebacterium tuberculostearicum in the sinuses.
Variation: Smokers and nonsmokers have different biota; lung microbiome composition differs in COPD, asthma, and cystic fibrosis patients.
Pharyngitis
Signs and Symptoms
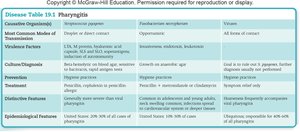
Pharyngitis is characterized by pain, inflammation of the throat, reddened or swollen mucosa, swollen tonsils, foul-smelling breath, and white packets on the throat walls (indicative of streptococcal disease). Bacterial pharyngitis is typically more painful and likely to be accompanied by fever, headache, and nausea.

Causative Agents
Pharyngitis can be caused by viruses (often those responsible for the common cold), mechanical irritation, or bacteria. The most serious cases are bacterial, primarily due to Streptococcus pyogenes and Fusobacterium necrophorum.
Streptococcus pyogenes: Pathogenesis and Virulence Factors
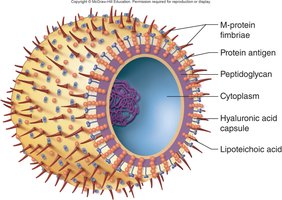
Streptococcus pyogenes is a gram-positive coccus that grows in chains, is nonmotile, and does not form endospores or capsules. It is a facultative anaerobe and survives in oxygen via a peroxidase system. Untreated infections can lead to serious complications such as scarlet fever (caused by erythrogenic toxin from bacteriophage-infected strains) and rheumatic fever (immunologic cross-reaction with heart muscle).
Virulence factors: Specialized polysaccharides, lipoteichoic acid (adherence), M protein (resists phagocytosis), hyaluronic acid capsule (adhesiveness).
Extracellular toxins: Streptolysin O and S (beta-hemolysis, tissue injury), erythrogenic toxin (rash, fever).
Transmission, Diagnosis, and Treatment
S. pyogenes is transmitted via respiratory droplets or direct contact with mucus. It is carried as normal biota by 15% of the population, with over 80 serotypes. Diagnosis involves rapid tests (antibody detection) and culturing on sheep blood agar (beta-hemolysis). Prevention relies on hygiene; treatment is typically penicillin or cephalexin for allergies.
Bronchiolitis
Pathophysiology and Causative Agents
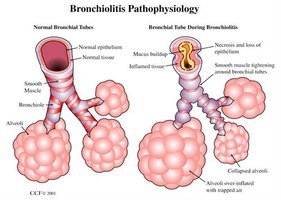
Bronchiolitis is the swelling of the bronchioles, primarily affecting children. It is most often caused by viruses such as respiratory syncytial virus (RSV), rhinoviruses, and influenza viruses, but can also result from chemical irritation (e.g., bronchiolitis obliterans).
Symptoms: Difficulty breathing due to inflamed and narrowed bronchioles.
Pathophysiology: Necrosis and loss of epithelium, mucus buildup, smooth muscle tightening, and over-inflated alveoli with trapped air.
The Common Cold
Causative Agents and Epidemiology
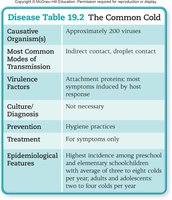
The common cold is caused by over 200 different viruses, including rhinoviruses (99 serotypes), coronaviruses, adenoviruses, and RSV. Transmission occurs via indirect contact and droplets. Symptoms include sneezing, scratchy throat, runny nose, and fever in children.
Prevention: Hygiene practices.
Treatment: Symptomatic relief only.
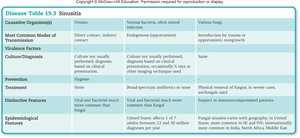
Sinusitis
Causative Agents and Treatment
Sinusitis can be caused by viruses, bacteria (often mixed infections), fungi, or noninfectious factors such as allergies and structural abnormalities. Treatment depends on the cause: broad-spectrum antibiotics for bacterial infections, antifungals or surgery for fungal infections.
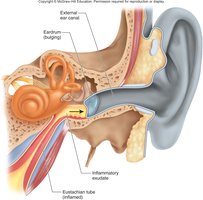
Acute Otitis Media
Pathogenesis and Treatment
Acute otitis media is often a complication of viral infections of the upper ear, leading to inflammation of the eustachian tubes, fluid buildup, and bacterial multiplication. Prevention includes vaccines (Prevnar, Hib), and treatment may involve "watchful waiting," antibiotics, or tympanic membrane tubes.
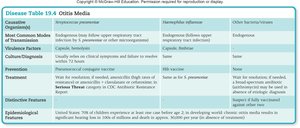
Diphtheria
Causative Agent and Pathogenesis
Diphtheria is caused by Corynebacterium diphtheriae, a non-spore-forming, gram-positive, club-shaped bacterium. Transmission occurs via droplets, direct contact, or fomites. The main virulence factor is the diphtheria exotoxin encoded by a bacteriophage.
Diagnosis: Tellurite medium (gray/black colonies).
Prevention: Diphtheria toxoid vaccine (DTP).
Treatment: Antitoxin plus penicillin or erythromycin.
Whooping Cough (Pertussis)
Causative Agent and Pathogenesis
Whooping cough is caused by Bordetella pertussis and transmitted via droplets. The disease progresses through incubation, catarrhal, paroxysmal, and recovery phases. Virulence factors include tracheal cytotoxin (disrupts cilia movement) and adenylate cyclase toxin (increases cAMP).
Diagnosis: Growth on Bordet-Gengou agar or BCYE plate.
Prevention: DTaP vaccine, antibiotic treatment for contacts.
Treatment: Erythromycin.

Influenza
Structure and Pathogenesis
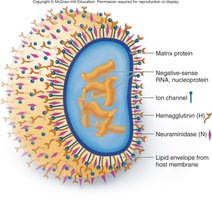
Influenza is a viral infection caused by Influenza A, B, and C viruses (Orthomyxoviridae). The virus has a lipoprotein envelope, glycoprotein spikes (hemagglutinin [H] and neuraminidase [N]), ion channels, and a segmented ssRNA genome.
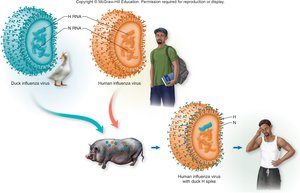
Antigenic drift: Mutation of glycoprotein genes, producing most seasonal strains.
Antigenic shift: RNA exchange between viruses, more likely to produce pandemic strains.
Pathogenesis: Virus binds ciliated cells, induces severe inflammation and "cytokine storm." Hemagglutinin binds host cell receptors; neuraminidase breaks down mucus and assists viral release.

Transmission, Diagnosis, Prevention, and Treatment
Influenza is transmitted via aerosols, droplets, and fomites. Diagnosis is often based on symptoms, with rapid tests (immunofluorescence, PCR, ELISA) and viral culture. Prevention includes vaccination (inactivated, live attenuated, recombinant). Treatment involves antiviral drugs (amantadine, rimantadine, zanamivir, oseltamivir).

Tuberculosis
Pathogenesis and Clinical Forms
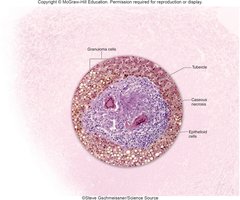
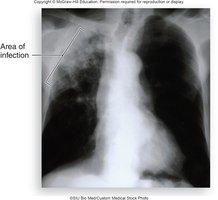
Tuberculosis is caused by Mycobacterium tuberculosis, an acid-fast bacillus with a waxy cell wall. The disease can be primary, secondary (reactivation), or extrapulmonary. Primary TB involves tubercle formation in the lungs; secondary TB is characterized by chronic symptoms and high mortality if untreated; extrapulmonary TB affects other organs.
Pathogenesis: Bacteria multiply inside macrophages, escape, and trigger cell-mediated immune responses. Tubercle formation and caseous necrosis are hallmarks.
Diagnosis and Treatment
Diagnosis relies on tuberculin testing (Mantoux Test), chest X-rays, blood testing (IGRA), culture, acid-fast staining, and PCR. Treatment of latent TB involves rifampin, rifapentine, or isoniazid; active TB requires a combination of drugs. MDR-TB and XDR-TB are resistant to multiple drugs and have high mortality rates.


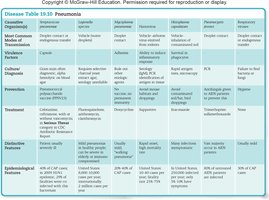
Pneumonia
Community-Acquired Pneumonia
Pneumonia is an inflammatory condition of the lungs with fluid-filled alveoli. It can be caused by bacteria, viruses, or fungi. Streptococcus pneumoniae is the most common cause of community-acquired bacterial pneumonia. Other agents include Legionella, Haemophilus influenzae, Mycoplasma pneumoniae, Chlamydophila pneumoniae, Histoplasma capsulatum, Hantavirus, and Pneumocystitis jiroveci.
Risk factors: Old age, underlying viral disease, diabetes, chronic alcohol/narcotic abuse.
Diagnosis: PCR, rapid antigen tests, culture.
Treatment: Antibiotics, antifungals, supportive care.
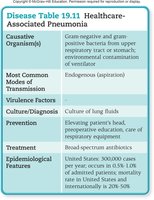
Healthcare-Associated Pneumonia
Healthcare-associated pneumonia affects up to 1% of hospitalized or institutionalized individuals, with a high mortality rate. Common causative agents include Pseudomonas aeruginosa, Acinetobacter baumanii, Streptococcus pneumoniae, Klebsiella pneumoniae, and Staphylococcus aureus (including MRSA).
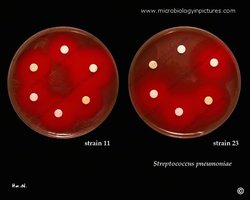
Laboratory Diagnosis: Optochin Disc Test
The optochin disc test is used for the presumptive identification of alpha-hemolytic Streptococcus pneumoniae. Optochin interferes with ATPase and ATP production in microorganisms. If susceptible to optochin, S. pneumoniae is likely.

COVID-19 (SARS-CoV-2)
Structure and Pathogenesis
SARS-CoV-2, the causative agent of COVID-19, is an enveloped virus with genes made from RNA surrounded by a protein capsid. The envelope makes the virus vulnerable to soap and alcohol. The 2002–2004 SARS outbreak was caused by a related coronavirus.
Prevention and Treatment
Prevention includes limiting exposure, mask use, distancing, isolation, and vaccination (RNA vaccines: Moderna, Pfizer; adenovirus vaccine: Johnson & Johnson). Treatment protocols are evolving and depend on disease severity.
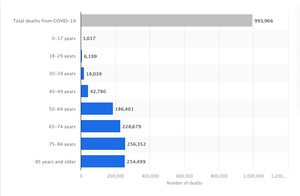
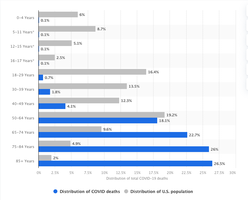
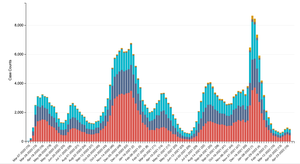
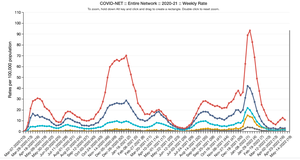
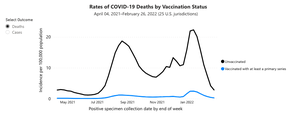
COVID-19 Epidemiology
COVID-19 has caused significant mortality, especially among older adults. Hospitalization and death rates are higher in older age groups, and vaccination reduces the risk of severe outcomes.
Summary Table: Respiratory Tract Pathogens
The following tables summarize key features of major respiratory tract infections, including causative agents, transmission, virulence factors, diagnosis, prevention, treatment, and epidemiological features.
