 Back
BackPractical Applications of Immunology: Vaccines and Monoclonal Antibodies
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Practical Applications of Immunology
Vaccines: Historical Development and Principles
Vaccines are a cornerstone of immunology, providing protection against infectious diseases by stimulating the immune system. The concept originated with variolation and was advanced by Jenner and Pasteur.
Variolation: Early method using material from smallpox scabs to induce immunity (1400s–1700s).
Vaccination: Jenner used cowpox to prevent smallpox (1798); Pasteur coined the term 'vaccination' (vacca = cow).
Vaccine: Suspension of organisms or their fractions that induce immunity.
Principles of Vaccination:
Provokes a primary immune response, leading to antibody and memory cell formation.
Enables a rapid, intense secondary response upon re-exposure.
Herd immunity: Immunity in most of the population reduces outbreaks.
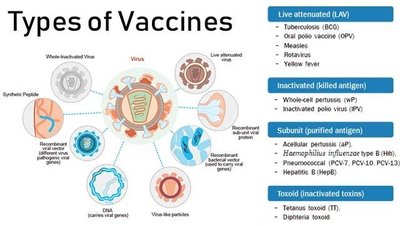
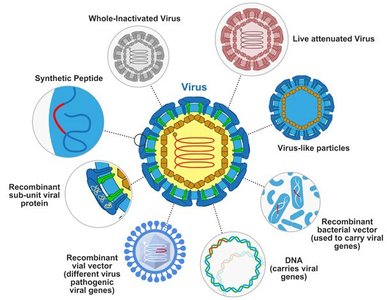
Types of Vaccines and Their Characteristics
Vaccines are classified based on their composition and method of action. Each type has distinct advantages and limitations.
Attenuated Vaccines: Weakened pathogens, closely mimic natural infection, confer lifelong immunity, not suitable for immunocompromised patients, risk of reversion to virulence.
Inactivated Vaccines: Whole microbes killed or inactivated, safer, require booster doses, induce mainly humoral immunity.
Subunit Vaccines: Use antigenic fragments; includes recombinant vaccines (produced by genetic modification), toxoids (inactivated toxins), virus-like particle (VLP) vaccines, polysaccharide vaccines, and conjugated vaccines.
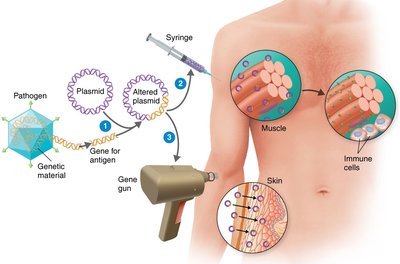
Nucleic Acid Vaccines: DNA or mRNA vaccines direct synthesis of protein antigens, stimulating both humoral and cellular immunity.
Recombinant Vector Vaccines: Avirulent viruses or bacteria genetically modified to deliver DNA coding for antigens.
CDC-Recommended Vaccines to Prevent Bacterial and Viral Diseases
The CDC recommends various vaccines to prevent bacterial and viral diseases. These recommendations are based on age, risk factors, and disease prevalence.
Bacterial Diseases
Disease(s) | Vaccine | Recommendation | Booster |
|---|---|---|---|
H. Influenzae type b meningitis | Polysaccharide from H. influenzae type b | Children 2-18 months | None recommended |
Meningococcal A C W Y meningitis | Purified polysaccharide from Neisseria meningitides | Age 11–12 years | At 16 years and for outbreak settings |
Meningococcal B meningitis | Purified polysaccharide from Neisseria meningitidis | Substantial risk; college freshmen in dorms | After 1 year; every 2–3 years if risk remains |
Pneumococcal pneumonia | Polysaccharide from Streptococcus pneumoniae | Adults with chronic diseases, people over 65, children 2–18 months | None if first dose ≥24 months |
Tetanus, diphtheria, pertussis | DTaP, Tdap, Td | Children 2–18 months, 4–6 years; single dose for 11–12 years and adults | Tdap or Td every 10 years |
Viral Diseases
Disease(s) | Vaccine | Recommendation | Booster |
|---|---|---|---|
Chickenpox (varicella) | Attenuated virus | Infants aged 12 months | Duration unknown |
COVID-19 | mRNA | Two dose series, ages vary | Recommended |
Dengue | Attenuated recombinant virus | Age 9–16 years in endemic areas | None recommended |
Hepatitis A | Inactivated virus | Children at age 1 year; risk groups | Protection ~10 years |
Hepatitis B | Virus antigen in yeast cells | Infants, children, risk groups | Protection ≥7 years; boosters uncertain |
Human Papillomavirus | Virus antigen in yeast/insect cells | Children ages 11–12 | Duration ≥5 years |
Influenza | Injected/inactivated or nasal/attenuated virus | Everyone over 6 months | Annual |
Measles | Attenuated virus | Infants aged 15 months; adults if exposed | As needed |
Mumps | Attenuated virus | Infants aged 15 months; adults if exposed | As needed |
Poliomyelitis | Inactivated virus | Children; adults as risk warrants | Duration unknown |
Rabies | Inactivated virus | Field biologists, veterinarians, exposed individuals | Every 2 years |
Rotavirus | Attenuated virus | Oral, infants up to 8 months | None recommended |
Rubella | Attenuated virus | Infants aged 15 months; females of childbearing age | As needed |
Smallpox | Attenuated vaccinia virus | Military, health care personnel | Protection 3–5 years |
Zoster (shingles) | Virus antigen in mammalian cells | Adults over 50; immunocompromised over 19 | None recommended |
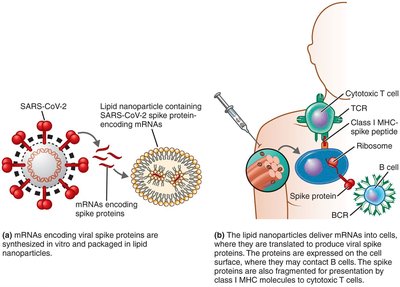
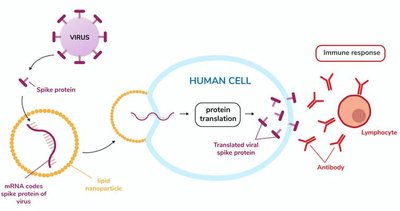
Mechanisms of Nucleic Acid Vaccines
Nucleic acid vaccines represent a modern approach, using DNA or mRNA to direct the synthesis of antigens within host cells, thereby stimulating immunity.
DNA Vaccines: Injected naked or encapsulated DNA into muscle; DNA is transcribed and translated to produce protein antigen.
mRNA Vaccines: mRNA enclosed in lipid nanoparticles is injected; directs synthesis of encoded antigen (e.g., COVID-19 spike protein).
Recombinant Vector Vaccines
Recombinant vector vaccines use genetically modified avirulent viruses or bacteria to deliver DNA coding for antigens, stimulating an immune response.
Vaccine Production, Administration, and Safety
Modern vaccine production methods avoid the need for animal hosts, utilizing plants and recombinant technology. Administration routes and adjuvants enhance effectiveness and safety.
Production: DNA, mRNA, and recombinant vector vaccines do not require animal hosts; plants are potential production systems.
Adjuvants: Additives (e.g., alum, monophosphoryl lipid A) improve vaccine effectiveness by activating innate immunity.
Administration: Oral, nasal, skin patch, and combination vaccines increase accessibility and effectiveness.
Safety: Vaccines are generally safe; rare cases of disease induction (e.g., oral polio vaccine); no evidence linking MMR to autism; mRNA vaccines have outstanding safety records.
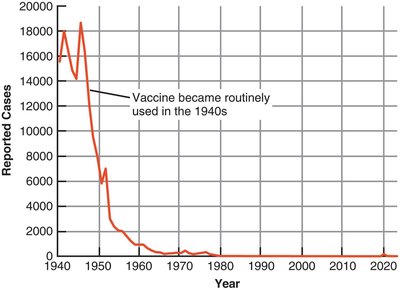
Impact of Vaccines on Disease Prevention
Vaccines have dramatically reduced the incidence of infectious diseases, saving millions of lives. However, some diseases persist due to low vaccination rates, need for boosters, and vaccine hesitancy.
Diphtheria: Before vaccine, >15,000 deaths in 1921; only 14 cases since 1996.
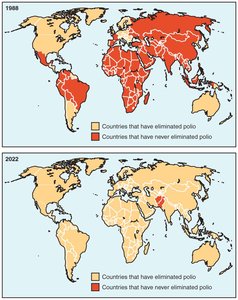
Measles and Rubella Initiative: Focused on disease elimination.
Global Polio Eradication Initiative: Polio eliminated in most countries; persists in Afghanistan and Pakistan.
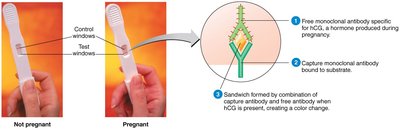
Monoclonal Antibodies: Production and Applications
Hybridoma Technology and Monoclonal Antibodies (Mabs)
Monoclonal antibodies are produced by hybridoma technology, combining a cancerous B cell with a normal antibody-producing B cell. This allows for the production of highly specific, uniform antibodies in large quantities.
Hybridoma: Fusion of myeloma cell and normal B cell; produces monoclonal antibodies.
Monoclonal Antibodies: Uniform, highly specific, used in diagnostics and therapy.
Applications: Diagnostic tools, treatments for multiple sclerosis, Crohn’s disease, psoriasis, cancer, asthma, arthritis, COVID-19.
Source: Often derived from mouse cells, which may cause side effects.
Summary Table: Types of Vaccines
Type | Example | Key Features |
|---|---|---|
Live Attenuated | Measles, Mumps, Rubella, Oral Polio | Strong, long-lasting immunity; risk for immunocompromised |
Inactivated | Influenza, Hepatitis A | Safe, requires boosters |
Subunit | Hepatitis B, HPV | Specific antigens, fewer side effects |
Toxoid | Diphtheria, Tetanus | Inactivated toxins, induce antitoxin immunity |
Conjugated | Haemophilus influenzae type b | Polysaccharide linked to protein, effective in young children |
Nucleic Acid | COVID-19 mRNA vaccines | Directs synthesis of antigen, stimulates both humoral and cellular immunity |
Recombinant Vector | Ebola vaccine | Uses modified virus/bacteria to deliver antigen gene |
Additional info: Modern vaccine development increasingly relies on recombinant and nucleic acid technologies, which allow rapid response to emerging pathogens and improved safety profiles.
