 Back
BackRespiratory System Infections: Anatomy, Defenses, and Microbial Diseases
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Respiratory System: Anatomy and Defenses
Basic Anatomy of the Respiratory Tract
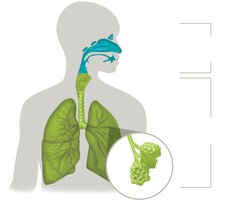
The respiratory tract is divided into upper and lower sections, each with distinct anatomical features and functions. Understanding these divisions is essential for recognizing how infections develop and spread.
Upper respiratory tract: Includes the mouth, nose, nasal cavity, pharynx, epiglottis, and larynx.
Lower respiratory tract: Comprises the trachea, bronchi, bronchioles, and alveoli, where gas exchange occurs.
Respiratory Tract Defenses
The respiratory system employs multiple defense mechanisms to prevent infection by inhaled pathogens and debris.
First line of defense: Mucociliary escalator—Ciliated mucous membranes trap and sweep debris toward the mouth; actions like coughing and sneezing help expel particles.
Second line of defense: Alveolar macrophages—Immune cells residing in alveoli that engulf and remove pathogens not trapped by the mucociliary escalator.
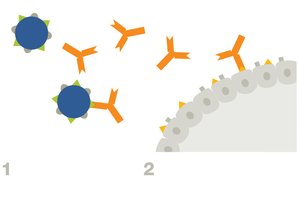
Third line of defense: Secretory IgA—Antibodies present in mucosal secretions that neutralize pathogens.

Normal Biota of the Respiratory Tract
The respiratory tract harbors a diverse community of resident microbiota, which play a protective role but can also become opportunistic pathogens under certain conditions.
Normal biota compete with potential pathogens for resources and space.
Some secrete antimicrobial peptides to inhibit pathogen growth.
Opportunistic pathogens include Streptococcus pyogenes, Haemophilus influenzae, Streptococcus pneumoniae, Neisseria meningitidis, and Staphylococcus aureus.
Respiratory Infections: Signs, Symptoms, and Diseases
Common Signs and Symptoms
Respiratory infections often present with a combination of the following clinical features:
Coughing
Stridor (high-pitched wheezing)
Dyspnea (shortness of breath)
Fatigue
Sneezing
Sore throat
Fever
Upper Respiratory Tract Diseases Caused by Microorganisms
Several diseases affect the upper respiratory tract, with the common cold and pharyngitis being the most prevalent.
The common cold ("rhinitis"): Primarily caused by viruses (see Chapter 6).
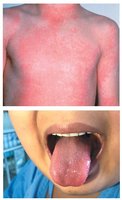
Pharyngitis: Inflammation of the throat, often with reddened mucosa and swollen tonsils. Causative agents include cold viruses and Streptococcus pyogenes.
Streptococcus pyogenes and Streptococcal Pharyngitis
Characteristics and Epidemiology
Streptococcus pyogenes is the most common bacterial cause of pharyngitis (strep throat). It is a Gram-positive, Group A streptococcus with a protective capsule.
Source: Humans (normal biota and asymptomatic carriers)
Transmission: Respiratory droplets
Seasonality: Most cases occur in winter and early spring
Clinical Presentation
Throat inflammation
Swollen cervical lymph nodes
Low-grade fever
Exudate (pus) in the throat or on tonsils

Diagnosis of Streptococcal Pharyngitis
Diagnosis involves a combination of clinical examination and laboratory testing:
Visual examination of the throat
Rapid strep test for bacterial antigens
Blood agar culture to identify S. pyogenes

Treatment and Prevention
Treatment: Penicillin-based drugs or macrolide antibiotics
Prevention: No vaccine available; good hand hygiene is recommended
Virulence Factors of Streptococcus pyogenes
S. pyogenes possesses several virulence factors that enhance its pathogenicity:
M protein: Facilitates attachment and evasion of phagocytosis
Hyaluronic acid capsule: Protects against immune detection
Extracellular toxins: Streptolysins, erythrogenic toxin (causes scarlet fever), and superantigens
Complications of S. pyogenes Infection
Scarlet fever: Characterized by a rash and high fever, resulting from erythrogenic toxin produced by bacteriophage-infected bacteria.
Rheumatic fever: An autoimmune complication affecting heart valves and joints. M proteins can trigger antibodies that cross-react with host tissues, leading to tissue damage.
Additional info: Rheumatic fever is a classic example of molecular mimicry, where immune responses to microbial antigens inadvertently target similar host proteins.
Lower Respiratory Tract Infections: Pneumonia
Pneumonia: Overview and Classification
Pneumonia is a leading cause of death in developing countries and is classified based on the causative agent and the context of acquisition.
By pathogen: Bacterial, viral, or fungal pneumonia
By acquisition:
Community-acquired pneumonia
Healthcare-acquired pneumonia (HCAP)
Hospital-acquired pneumonia (HAP)
Ventilator-associated pneumonia (VAP)
Typical pneumonia: Presents with consolidation (fluid-filled alveoli visible as white areas on X-ray), often caused by Streptococcus pneumoniae. Atypical pneumonia: Lacks consolidation; often caused by Mycoplasma pneumoniae and other agents.
Additional info: Consolidation refers to the merging of alveoli due to fluid accumulation, impairing gas exchange.
Healthcare-Associated Pneumonia
Hospital-acquired pneumonia (HAP) is a lower respiratory infection acquired during a hospital stay and is a common healthcare-associated infection (HAI).
Often caused by multidrug-resistant organisms
Prevention includes infection control practices and minimizing ventilator use when possible
