 Back
BackSkin and Eye Infections: Structure, Defenses, and Microbial Diseases
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Overview of Skin Structure, Defenses, and Afflictions
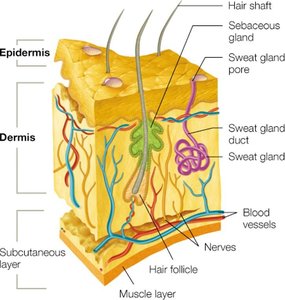
Skin Structure and Protective Functions
The skin is the largest organ of the human body and serves as a primary barrier against infectious agents. It is composed of several layers, each with specialized cells and functions that contribute to its protective role.
Epidermis: Outermost layer, consisting of tightly packed dead cells on the surface and living keratinocytes beneath. Keratinocytes produce keratin, a protein that strengthens the skin and provides water resistance.
Dermis: Thicker layer beneath the epidermis, composed of connective tissue, dermal fibroblasts, collagen fibers, immune cells, blood vessels, nerves, hair follicles, sweat gland ducts, and sebaceous glands.
Subcutaneous Layer: Not technically part of the skin, but closely associated. Contains fat cells, nerves, and blood vessels, providing insulation and cushioning.
Skin Defense Mechanisms
Melanin: Pigment with antimicrobial properties.
Perspiration: Acidic pH and high salt content inhibit microbial growth; sweat washes away microbes.
Lysozyme: Enzyme in sweat that breaks down bacterial peptidoglycan.
Sebum: Oily substance from sebaceous glands; contains low pH lipids and proteins that moisturize and inhibit microbes. Some bacteria metabolize sebum, producing toxic fatty acids.
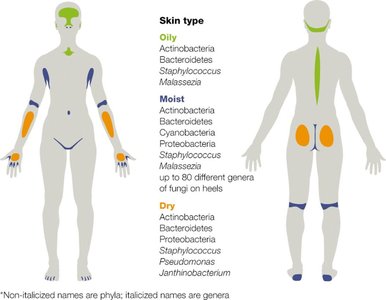
Skin Microbiome
The skin hosts a diverse microbiome, with microbial populations varying by site (oily, moist, dry). Normal microbiota reside on the epidermis, sweat glands, sebaceous glands, and hair follicles. Common residents include:
Gram-positive cocci: Staphylococcus species
Gram-negative rods: Pseudomonas, Janthinobacterium species
Fungi: Malassezia species
Factors influencing the skin microbiome include environment, occupation, antibiotic use, age, cosmetics, hygiene products, clothing, and hormone levels.
Skin Lesions and Rashes: Clinical Terminology
Understanding skin lesions is essential for diagnosis. Lesions are changes or abnormalities in the skin, classified as primary (directly associated with a disease) or secondary (develop from primary lesions or other causes).
Vesicle: Small, elevated lesion filled with clear fluid (e.g., chickenpox).
Bulla: Large vesicle (>0.5 cm, e.g., blister).
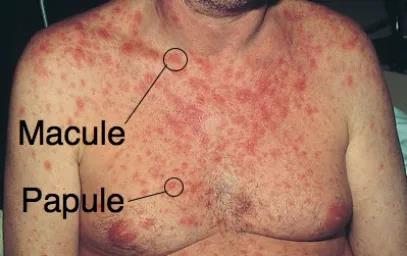
Macule: Flat, discolored area (e.g., freckles).
Papule: Raised, solid lesion (<0.5 cm, e.g., wart).
Pustule: Raised lesion with pus (e.g., acne).
Cyst: Closed, fluid-filled sac deeper in the skin (e.g., nodular cystic acne).
Maculopapular rash: Slightly raised papules overlying macules (e.g., rubella, rubeola).





Secondary lesions include:
Crust: Dried exudate or plasma (e.g., impetigo).
Scale: Flaking of outer epidermal layers (e.g., athlete’s foot, psoriasis).
Purpura: Large purple spots from subcutaneous bleeding (3–10 mm).
Petechiae: Small pinpoint spots (<3 mm) from capillary bursts.
Ulcer: Open sore from destruction of skin layers (e.g., cutaneous anthrax).




Viral Skin Infections
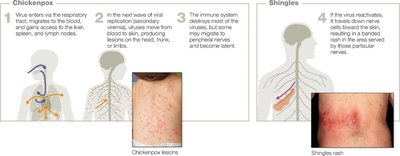
Chickenpox and Shingles
Chickenpox and shingles are caused by the varicella-zoster virus (Herpesviridae family). Chickenpox is highly contagious and spreads via respiratory droplets or direct contact with lesions. After initial infection, the virus can become latent in peripheral nerves and reactivate later as shingles, especially in older adults.
Chickenpox: Fever and itchy vesicular rash; more severe in adults.
Shingles: Reactivation of latent virus; painful, banded rash on one side of the body; risk of postherpetic neuralgia (chronic pain).
Prevention: Varicella vaccine (chickenpox), Shingrix vaccine (shingles for adults over 50).

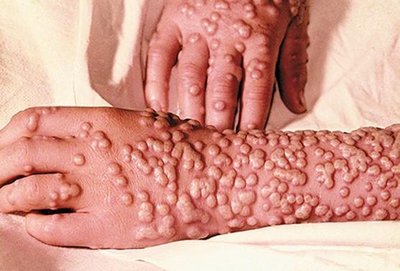
Smallpox
Smallpox, caused by the variola major virus, had a 30% mortality rate and was eradicated worldwide by 1980 through vaccination. It was highly contagious, transmitted by respiratory droplets or fomites, and characterized by a deep, domed rash with possible scarring.
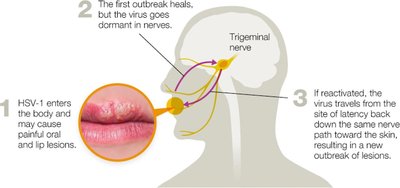
Herpes Simplex Virus (HSV-1)
HSV-1 causes oral herpes (cold sores) and is highly prevalent. The virus becomes latent in the trigeminal nerve and can reactivate due to stress, UV light, or hormonal changes. Transmission occurs via saliva or contaminated objects.
Symptoms: Painful, itchy vesicular lesions on lips; initial infection may include sore throat or flu-like symptoms.
Treatment: No cure; antiviral medications reduce outbreak frequency and severity.

Maculopapular Viral Rashes
Several viral infections cause maculopapular rashes, including measles (rubeola), rubella (German measles), fifth disease, roseola, and hand, foot, and mouth disease.
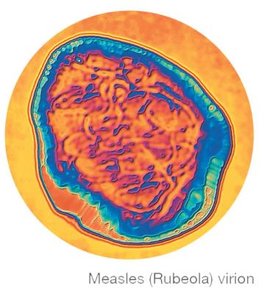
Measles (Rubeola)
Etiological agent: Measles virus (Paramyxoviridae family).
Transmission: Respiratory droplets; highly contagious.
Symptoms: Fever, sore throat, dry cough, Koplik’s spots, maculopapular rash starting on the face.
Complications: Encephalitis, pneumonia, death.
Prevention: MMR vaccine.

Rubella (German Measles)
Etiological agent: Rubella virus (Togaviridae family).
Symptoms: Rash starting on the face, fever, swollen lymph nodes, joint aches.
Complications: Congenital rubella syndrome (CRS) in infants if contracted during pregnancy.
Prevention: MMR vaccine (not for pregnant women or immunosuppressed individuals).

Fifth Disease
Etiological agent: Parvovirus B19.
Symptoms: "Slapped cheek" rash, mild illness, possible lacy rash on trunk and limbs.
Complications: Risk for pregnant women, sickle-cell anemia, immunodeficiency disorders.

Roseola
Etiological agent: Human herpes viruses 6 and 7.
Symptoms: Sudden high fever, followed by a body-wide rash.

Hand, Foot, and Mouth Disease
Etiological agents: Coxsackievirus A16, Enterovirus 71.
Symptoms: Blister-like sores in the mouth, lesions on hands and feet.

Warts (Papillomaviruses)
Warts are caused by over 50 types of papillomaviruses, which deregulate host cell division. Most warts are harmless and self-resolve, but can be treated by cryogenic, chemical, or laser removal.

Bacterial Skin Infections
Acne (Propionibacterium acnes)
Acne is a common skin infection, especially in adolescents, caused mainly by Propionibacterium acnes (Gram-positive rods). It results from clogged pores, sebum production, and inflammation.
Treatment: Retinoids, antibiotics, benzoyl peroxide, photodynamic therapy, laser, or heat pulses.

Staphylococcus aureus Skin Diseases
Staphylococcus aureus is a leading cause of skin infections, producing various virulence factors (e.g., coagulase, catalase, hemolysins, exfoliative toxins). It can cause impetigo, erysipelas, cellulitis, folliculitis, and scalded skin syndrome.
Impetigo: Superficial, pus-filled vesicles that crust over into honey-colored lesions; highly contagious.
Cellulitis: Infection of lower dermis and subcutaneous fat; red, swollen, painful skin; can be life-threatening.
Scalded Skin Syndrome: Exfoliative toxins cause the outer epidermal layer to peel in sheets.



Methicillin-Resistant Staphylococcus aureus (MRSA)
MRSA is resistant to methicillin and other beta-lactam antibiotics due to modified penicillin-binding proteins. Treatment includes vancomycin and other antibiotics, but resistance is emerging. Prevention relies on strict hygiene and antisepsis in healthcare settings.
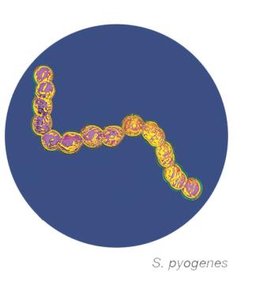
Streptococcus pyogenes Skin Infections
Streptococcus pyogenes (Group A Streptococcus, GAS) can cause impetigo, cellulitis, necrotizing fasciitis (flesh-eating disease), and streptococcal toxic shock syndrome. It produces numerous virulence factors, including M-protein, hemolysins, and exotoxins.

Pseudomonas aeruginosa Infections
Pseudomonas aeruginosa is a Gram-negative rod that causes opportunistic infections, especially in burn and wound patients. It forms biofilms, produces pigments (e.g., pyocyanin), and is highly resistant to antibiotics and disinfectants.
Wound infections: Greenish-blue pus, risk of systemic infection.
Otitis externa (swimmer’s ear): Infection of the outer ear canal, often after swimming in contaminated water.


Gas Gangrene (Clostridium perfringens)
Gas gangrene is caused by Clostridium perfringens, an anaerobic, endospore-forming Gram-positive rod. It infects deep wounds, producing gas and toxins that destroy tissue. Treatment includes antibiotics, debridement, and hyperbaric oxygen therapy.
Cutaneous Anthrax (Bacillus anthracis)
Cutaneous anthrax is caused by Bacillus anthracis, a Gram-positive, endospore-forming bacterium. It enters through skin abrasions, forming a painless black ulcer (eschar). Untreated cases can be fatal.
Fungal Skin Infections (Mycoses)
Cutaneous Mycoses
Fungal skin infections are usually superficial and caused by Candida, Piedraia, Trichosporon, Malassezia, and dermatophytes (e.g., Trichophyton, Microsporum, Epidermophyton species). Dermatophytes break down keratin, causing brittle skin, hair, and nails.
Yeast Infections (Cutaneous Candidiasis)
Caused by Candida albicans, a normal skin and GI tract resident. Infections occur in moist, friction-prone areas (e.g., underarms, groin, under breasts). Symptoms include a bright red macular rash, white pustules, and itching or burning. Treatment involves keeping the area dry and using topical antifungals.
Tinea Infections (Ringworm)
Tinea infections are not caused by worms but by fungi. Types include tinea pedis (athlete’s foot), tinea cruris (jock itch), tinea capitis (scalp), tinea unguium (nails), and tinea corporis (body). Transmission occurs via skin contact, fomites, or animals. Treatment includes topical or oral antifungals.
Parasitic Skin Infections
Cutaneous Leishmaniasis
Caused by Leishmania species (protozoa), transmitted by sand fly bites. Cutaneous leishmaniasis presents as painless skin ulcers, which may persist and scar. Prevention involves avoiding sand fly bites; treatment includes antiprotozoal drugs.
Structure, Defenses, and Infections of the Eyes
Eye Structure and Defenses
The eye is protected by the cornea (outermost layer), conjunctiva (membrane covering the eyeball and eyelids), thick outer wall, and tears containing lysozyme and lactoferrin. The ocular microbiome consists of bacteria adapted to the conjunctiva and cornea.
Conjunctivitis (Pink Eye)
Conjunctivitis is inflammation of the conjunctiva, presenting as red or pink eyes, swelling, and discharge. It can be non-contagious (allergens, chemicals) or contagious (viral or bacterial).
Viral conjunctivitis: Most commonly caused by adenoviruses; watery discharge; self-resolving.
Bacterial conjunctivitis: Caused by Haemophilus influenzae, Staphylococcus, Streptococcus, or Moraxella; pus-like discharge; treated with antibiotics.
Neonatal conjunctivitis: Caused by Neisseria gonorrhoeae or Chlamydia trachomatis; prevented by antibiotic drops at birth.
Trachoma
Trachoma, caused by Chlamydia trachomatis, is the leading cause of preventable blindness worldwide. Repeated infections scar the conjunctiva, causing eyelashes to damage the cornea. Prevention includes hygiene and sanitation; treatment is with azithromycin and surgery if needed.
Keratitis
Keratitis is severe inflammation of the cornea, more serious than conjunctivitis. It can be caused by viruses (HSV-1), bacteria (P. aeruginosa, S. aureus), fungi (Fusarium, Aspergillus, Candida), or parasites (Acanthamoeba, Onchocerca volvulus). Symptoms include pain, blurred vision, and discharge. Treatment depends on the causative agent and may require urgent medical intervention.
