 Back
BackStaphylococcus aureus: Clinical Features, Pathogenesis, and Treatment
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
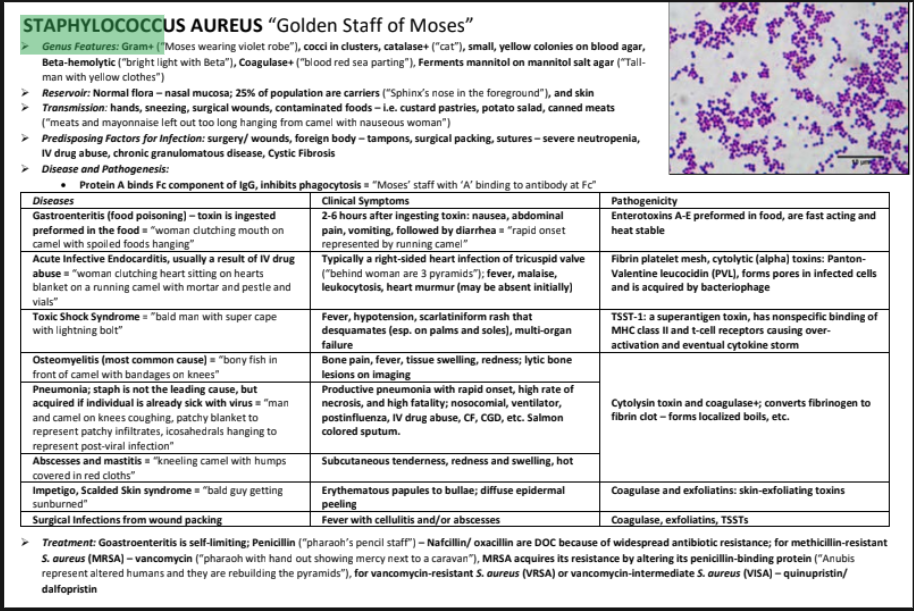
Staphylococcus aureus
Genus Features and Identification
Staphylococcus aureus is a Gram-positive coccal bacterium, commonly found in clusters. It is catalase-positive and forms small, yellow colonies on blood agar. It is notable for its ability to ferment mannitol on mannitol salt agar and for its beta-hemolytic activity, which is visible as clear zones around colonies on blood agar.
Gram-positive: Thick peptidoglycan cell wall, stains violet in Gram stain.
Catalase-positive: Produces catalase enzyme, distinguishing it from Streptococcus species.
Beta-hemolysis: Complete lysis of red blood cells on blood agar.
Mannitol fermentation: Produces acid, turning mannitol salt agar yellow.
Reservoirs and Transmission
S. aureus is part of the normal flora of the nasal mucosa and skin. About 25% of the population are carriers. Transmission occurs via direct contact (hands), respiratory droplets (sneezing), surgical wounds, and contaminated foods.
Reservoir: Nasal mucosa, skin.
Transmission: Hands, sneezing, surgical wounds, contaminated foods (e.g., custard pastries, potato salad, canned meats).
Predisposing Factors for Infection
Individuals with surgical wounds, severe neutropenia, IV drug abuse, chronic granulomatous disease, or cystic fibrosis are at increased risk for S. aureus infection.
Surgery and wound packing
Severe neutropenia
IV drug abuse
Chronic granulomatous disease
Cystic fibrosis
Disease and Pathogenesis
S. aureus produces several virulence factors that contribute to its pathogenicity:
Protein A: Binds Fc region of IgG, inhibiting phagocytosis.
Coagulases: Convert fibrinogen to fibrin, promoting abscess formation.
Exfoliative toxins: Cause skin peeling in scalded skin syndrome.
TSST-1: Superantigen toxin causing toxic shock syndrome.
Panton-Valentine leukocidin (PVL): Forms pores in leukocytes, leading to cell lysis.
Clinical Diseases and Symptoms
S. aureus is associated with a wide range of diseases, each with distinct clinical presentations and pathogenic mechanisms.
Diseases | Clinical Symptoms | Pathogenicity |
|---|---|---|
Gastroenteritis (food poisoning) | 2-6 hours after ingesting toxin: nausea, abdominal pain, vomiting, followed by diarrhea | Enterotoxins A-E preformed in food, fast acting and heat stable |
Acute Infective Endocarditis (IV drug abuse) | Fever, malaise, leukocytosis, heart murmur (may be absent initially) | Fibrin platelet mesh, cytolytic (alpha) toxins: PVL, forms pores in infected cells |
Toxic Shock Syndrome | Fever, hypotension, scarlatiniform rash (esp. on palms and soles), multi-organ failure | TSST-1: superantigen toxin, nonspecific binding of MHC class II and T-cell receptors, cytokine storm |
Osteomyelitis (most common cause) | Bone pain, fever, tissue swelling, redness; lytic bone lesions on imaging | Cytolysin toxin and coagulases; lytic bone lesions |
Pneumonia (post-viral, nosocomial, etc.) | Productive pneumonia with rapid onset, high fatality; salmon-colored sputum | Cytolysin toxin and coagulase; converts fibrinogen to fibrin clot |
Abscesses and mastitis | Subcutaneous tenderness, redness, swelling, hot | Cytolysin toxin and coagulases; localized boils |
Impetigo, Scalded Skin Syndrome | Erythematous papules to bullae; diffuse epidermal peeling | Coagulase and exfoliative toxins |
Surgical infections from wound packing | Fever with cellulitis and/or abscesses | Coagulase, exfoliative, TSSTs |
Treatment and Antibiotic Resistance
Gastroenteritis caused by S. aureus is self-limiting. For other infections, penicillin was historically used, but resistance is widespread. Nafcillin and oxacillin are now preferred. Methicillin-resistant S. aureus (MRSA) is treated with vancomycin. MRSA acquires resistance by altering its penicillin-binding protein. For vancomycin-resistant S. aureus (VRSA) or vancomycin-intermediate S. aureus (VISA), quinupristin/dalfopristin are used.
Penicillin: Historically used, now limited due to resistance.
Nafcillin/Oxacillin: Drugs of choice for most infections.
Vancomycin: Used for MRSA.
Quinupristin/Dalfopristin: Used for VRSA/VISA.
Example: MRSA resistance is due to altered penicillin-binding protein, making beta-lactam antibiotics ineffective.
Additional info: S. aureus is a major cause of nosocomial infections and is notable for its ability to form biofilms on medical devices, contributing to persistent infections.
