 Back
BackSuperficial, Cutaneous, and Subcutaneous Mycoses: Pathogenic Fungi and Fungal Intoxications
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Superficial, Cutaneous, and Subcutaneous Mycoses
Overview of Superficial, Cutaneous, and Subcutaneous Mycoses
Superficial, cutaneous, and subcutaneous mycoses are the most commonly reported fungal diseases in humans. These infections are generally opportunistic, affecting the skin, nails, and hair, and are typically localized at or near the body surface. They are acquired through person-to-person contact or environmental exposure and are rarely life-threatening, though they can cause chronic or recurring infections.
Superficial mycoses affect the outermost layers of skin and hair.
Cutaneous mycoses invade deeper into the epidermis, hair, and nails.
Subcutaneous mycoses involve the dermis, subcutaneous tissues, muscle, and fascia, usually following traumatic implantation of the fungus.

Superficial Mycoses: Dermatophytoses
Dermatophytoses are infections of the skin, nails, or hair caused by dermatophytes, a group of fungi that utilize keratin as a nutrient source. These infections, previously called "ringworms," are characterized by their ability to colonize dead tissues and may trigger immune responses that damage living tissues. Dermatophytes can spread from person to person.
Diagnosis: Identification of hyphae or arthroconidia in patient samples.
Treatment: Limited infections are treated with topical antifungals; widespread or chronic cases may require oral agents such as terbinafine or griseofulvin.
Common Dermatophytoses
Disease | Agents | Common Signs | Source |
|---|---|---|---|
Tinea pedis (athlete's foot) | Trichophyton rubrum, T. mentagrophytes var. interdigitale, Epidermophyton floccosum | Red, raised lesions on and around toes and soles; webbing between toes heavily infected | Human reservoirs in toe webbing; carpeting holding infected skin cells |
Tinea cruris (jock itch) | T. rubrum, T. mentagrophytes var. interdigitale, E. floccosum | Red, raised lesions on groin and buttocks | Usually spreads from the feet |
Tinea unguium (onychomycosis) | T. rubrum, T. mentagrophytes var. interdigitale | Patches or pits on nail surface; yellowing and thickening of distal nail plate | Humans |
Tinea corporis | T. rubrum, Microsporum gypseum, M. canis | Red, ringlike lesions on skin surfaces | Other body sites, contaminated soil or animals |
Tinea capitis | M. canis, M. gypseum, T. equinum, T. verrucosum, T. tonsurans, T. violaceum, T. schoenleinii | Lesions on scalp, hair loss, crusts (favus) | Humans, contaminated soil or animals |

Superficial Mycoses: Pityriasis
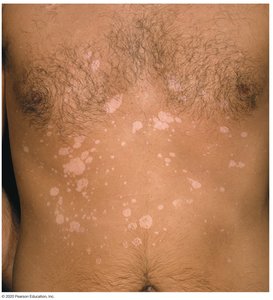
Pityriasis is caused by Malassezia furfur, a normal member of the skin microbiome. It is characterized by depigmented or hyperpigmented patches of scaly skin. Diagnosis is based on the presence of budding yeast and short hyphal forms in clinical samples. Superficial infections are treated with topical antifungals, while extensive infections may require oral therapy. Relapses are common.
Cutaneous and Subcutaneous Mycoses
Overview of Cutaneous and Subcutaneous Mycoses
These mycoses are less common than superficial infections and typically require traumatic introduction of fungi beneath the outer skin layer. Most lesions remain localized to subepidermal tissues. The main types include chromoblastomycosis, phaeohyphomycosis, mycetomas, and sporotrichosis.
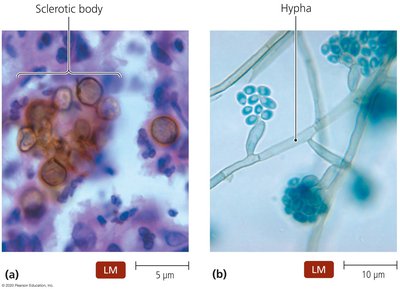
Chromoblastomycosis and Phaeohyphomycosis
Both are caused by dark-pigmented ascomycetes. Chromoblastomycosis is caused by Fonsecaea, Phialophora, and Cladophialophora, while phaeohyphomycosis is caused by Alternaria, Exophiala, Wangiella, and Cladophialophora. These infections are rare but more common in people who work with soil. Chromoblastomycosis produces progressively worsening skin lesions, while phaeohyphomycosis often involves the nasal passages and sinuses, especially in allergy sufferers and immunocompromised patients. Diagnosis is based on the morphology of fungal cells in tissue samples, and both diseases are difficult to treat.

Mycetomas
Mycetomas are tumorlike infections caused by mycelial fungi in the division Ascomycota, including Madurella, Pseudallescheria, Exophiala, and Acremonium. These fungi are found in soil and are introduced via wounds from contaminated plant material. Mycetomas are most prevalent near the equator and can cause nodules that worsen and spread, potentially leading to bone destruction and permanent deformity. Diagnosis is based on symptoms and the presence of fungi in patient samples. Treatment requires surgical removal followed by long-term antifungal therapy.

Sporotrichosis
Sporotrichosis is caused by Sporothrix schenckii and is usually limited to the arms and legs. The fungus is found in soil, and those who work with plant material are at highest risk. Most infections occur in Latin America, Mexico, and Africa. The disease initially produces nodular lesions, which may spread along lymphatic vessels. Diagnosis is based on patient history, clinical signs, and observation of dimorphic fungi in culture. It is effectively treated with topical agents, and prevention involves wearing protective clothing.

Fungal Intoxications and Allergies
Fungal Intoxications
Some fungi produce mycotoxins or cause allergies. Fungal mycotoxins cause toxicosis, which can be classified as:
Mycotoxicosis: Caused by ingestion of mycotoxins, often present in contaminated grains or vegetables. Aflatoxins are the best-known mycotoxins, which are carcinogenic and can cause liver damage and cancer.
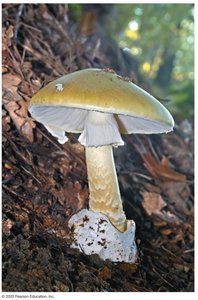
Mycetismus (mushroom poisoning): Results from eating toxic mushrooms. The deadliest toxins are produced by the "death cap" mushroom (Amanita phalloides), which damages cell structure and inhibits mRNA synthesis, leading to liver damage.
Other Deadly Mushrooms and Treatment
Gyromitra esculenta causes diarrhea, convulsions, and death.
Cortinarius genitalis causes thirst, nausea, and kidney failure.
Some mushrooms, such as Psilocybe cubensis and Amanita muscaria, produce hallucinogenic toxins.
Treatment for mushroom poisoning includes induced vomiting, administration of activated charcoal, and, in severe cases, liver transplantation.
Self-Assessment Questions
What nutrient source do dermatophytes use? Keratin.
Which infection produces depigmented or hyperpigmented patches of scaly skin? Pityriasis.
What does the image of nodular lesions along the arm show? Sporotrichosis.
