 Back
BackUrinary and Reproductive System Infections: Microbiology Study Guide
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Urinary and Reproductive System Infections
Overview
This chapter explores the microbiology of infections affecting the urinary and reproductive systems, focusing on the causative agents, clinical features, epidemiology, diagnosis, treatment, and prevention of urinary tract infections (UTIs) and sexually transmitted infections (STIs).
Urinary Tract Infections (UTIs)
Anatomy of the Urinary System
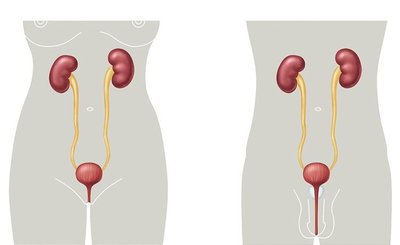
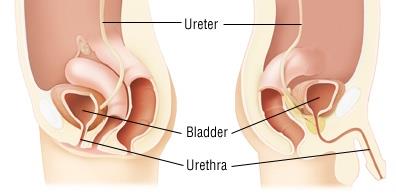
The urinary system consists of two kidneys, two ureters, one bladder, and one urethra. There are anatomical differences between males and females that influence infection risk.
Kidneys: Filter blood and produce urine.
Ureters: Transport urine from kidneys to bladder.
Bladder: Stores urine.
Urethra: Conducts urine out of the body; shorter in females, increasing UTI risk.
Microbiome and Infection Susceptibility
The urinary tract harbors a diverse microbiome, which varies by site, age, sex, and health status.
Shifts in the urinary microbiome can contribute to disease.
Types and Sites of UTIs
Urethritis: Inflammation of the urethra.
Cystitis: Inflammation of the bladder (commonly referred to as a UTI).
Ureteritis: Inflammation of the ureters.
Pyelonephritis: Inflammation of the kidneys; can lead to renal failure and bacteremia.
Lower UTIs (urethritis, cystitis) are usually less severe and may resolve with short treatment. Upper UTIs (ureteritis, pyelonephritis) are more serious and can be life-threatening if untreated.
Etiology and Epidemiology of UTIs
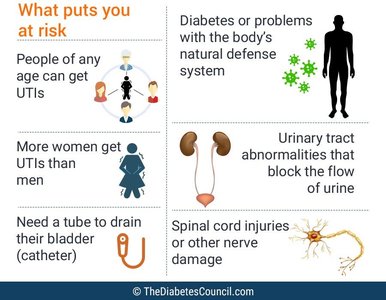
UTIs are a major healthcare issue, accounting for ~10 million doctor visits annually in the U.S.
1 in 2 women will experience a UTI in their lifetime.
Bacteria are the most common cause, especially Uropathogenic Escherichia coli (UPEC) and Staphylococcus saprophyticus.
Risk factors include anatomical differences, catheterization, urinary tract abnormalities, and immune compromise.
Complicated vs. Uncomplicated UTIs
Uncomplicated UTIs: Occur in healthy individuals with normal urinary tracts; respond well to therapy.
Complicated UTIs: Occur in individuals with catheters, anatomical abnormalities, or underlying health conditions; more likely to recur and resist treatment.
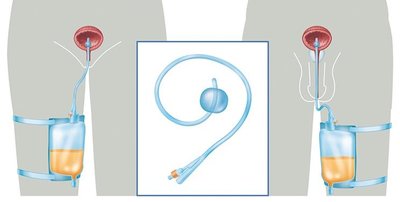
Catheter-Associated UTIs (CAUTIs)
Urinary catheters are tubes inserted to drain urine, often used in hospitalized or immobile patients.
Catheters increase UTI risk by introducing bacteria and providing surfaces for biofilm formation.
CAUTIs account for 70–80% of complicated UTIs and are a leading cause of healthcare-associated infections.

Clinical Presentation, Diagnosis, and Prevention
Lower UTI symptoms: Dysuria (painful urination), frequent urge, cloudy or foul-smelling urine, lower abdominal pain.
Upper UTI symptoms: Fever, nausea, vomiting, severe flank pain, risk of kidney damage.
Diagnosis: Urinalysis for white blood cells and culture; treated with antibiotics.
Prevention: Good hygiene, adequate hydration, urinating after sex, minimizing catheter use.

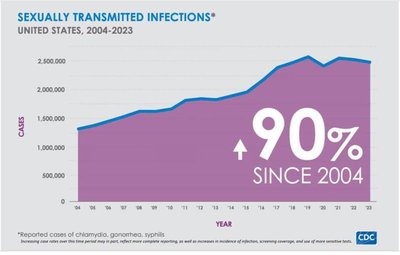
Sexually Transmitted Infections (STIs)
Overview and Transmission
STIs are infections primarily transmitted through sexual contact, affecting the urinary and reproductive systems. They can be caused by bacteria, viruses, or eukaryotic parasites.
Transmission occurs via mucous membranes, genital secretions, skin-to-skin contact, and sometimes non-sexual routes (e.g., mother to child, blood products).
General Symptoms and Epidemiology
Common symptoms: Dysuria, unusual discharge, sores, rash, pain during intercourse, bleeding between periods.
Most STIs are asymptomatic, facilitating their spread.
Incubation period: Symptoms, if present, usually develop within 2–30 days of exposure.

Major Causative Agents of STIs
Type | Examples |
|---|---|
Bacterial | Chlamydia (Chlamydia trachomatis), Gonorrhea (Neisseria gonorrhoeae), Syphilis (Treponema pallidum) |
Viral | Herpes simplex virus (HSV), Human papilloma virus (HPV), Human immunodeficiency virus (HIV) |
Eukaryotic | Trichomoniasis (Trichomonas vaginalis), Pubic lice, Scabies |
Bacterial STIs
Chlamydia (Chlamydia trachomatis)
Gram-negative, obligate intracellular pathogen lacking a peptidoglycan cell wall.
Most common bacterial STI worldwide; often asymptomatic ('silent epidemic').
Transmitted via sexual contact and from mother to child during birth.
Infects mucosal epithelial cells of the urogenital tract, rectum, conjunctiva, and pharynx.
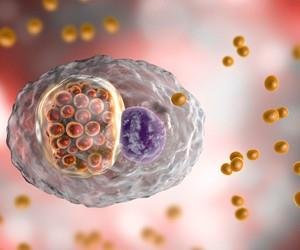
Life Cycle
Alternates between infectious elementary bodies (enter/exit host cells) and replicative reticulate bodies (grow inside host cells).
Both forms reside within a host cell phagosome (inclusion).

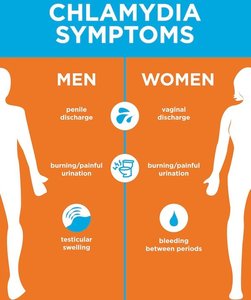
Clinical Features and Complications
Asymptomatic in ~75% of women and 50% of men.
Symptoms (if present): Dysuria, discharge, testicular or pelvic pain, bleeding between periods.
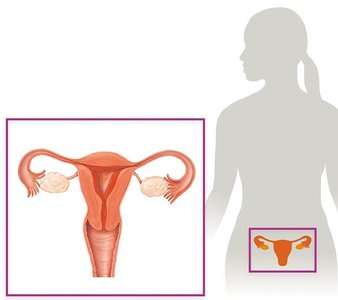
Complications (if untreated): Pelvic inflammatory disease (PID), infertility, ectopic pregnancy, chronic pain, neonatal conjunctivitis or pneumonia.
Lymphogranuloma Venereum (LGV)
Invasive, ulcerative STI caused by certain C. trachomatis biovars.
Stages: Painless ulcer → swollen lymph nodes (buboes) → chronic inflammation, scarring, abscesses.

Diagnosis and Treatment
Diagnosis: Nucleic acid amplification tests (NAATs) on urine or swabs.
Treatment: Early antibiotics are highly effective; late treatment does not reverse complications.
All sexual partners from the past 60 days must be treated.
Gonorrhea (Neisseria gonorrhoeae)
Gram-negative diplococcus; human-restricted pathogen.
Transmitted via sexual contact; infects mucous membranes (urethra, cervix, rectum, pharynx, conjunctiva).
Many infections are asymptomatic, especially in women.
Symptoms: Dysuria, purulent discharge, pelvic/testicular pain, abnormal bleeding.
Complications: PID, infertility, disseminated gonococcal infection (DGI), neonatal blindness.
Diagnosis: NAATs, culture, Gram stain.
Treatment: Antibiotics, but resistance is increasing; all partners must be treated.

Syphilis (Treponema pallidum)
Gram-negative spirochete; causes chronic, systemic infection.
Transmitted by contact with syphilitic chancre, blood, or from mother to fetus (congenital syphilis).
Stages:
Primary: Painless chancre at infection site.
Secondary: Rash, mucous patches, systemic symptoms.
Tertiary: Gummas, cardiovascular and neurological damage; can be fatal.
Diagnosis: Serology, NAATs, clinical features.
Treatment: Early antibiotics are curative; late treatment does not reverse damage.
Eukaryotic STI: Trichomoniasis (Trichomonas vaginalis)
Motile, flagellated protozoan; most common curable STI.
Often asymptomatic, especially in men.
Symptoms (if present): Foul-smelling, frothy vaginal discharge, genital redness, burning, itching, dysuria.
Complications: Premature labor, low-birth-weight babies, increased susceptibility to other STIs.
Diagnosis: Wet mount, NAAT.
Treatment: Antimicrobials; all partners must be treated.
Viral STIs
Herpes Simplex Virus (HSV)
Two types: HSV-1 (oral, sometimes genital), HSV-2 (genital).
Lifelong infection; virus establishes latency in peripheral nerves.
Symptoms: Painful blisters/ulcers, recurrent outbreaks, flu-like symptoms during first episode.
Transmission: Direct contact with skin, mucosa, or fluids; can occur without visible lesions.
Treatment: Antivirals suppress symptoms and transmission but do not cure.
Human Papilloma Virus (HPV)
Most common STI; >200 types, ~40 sexually transmitted.
Low-risk types cause warts; high-risk types (16, 18) cause cancers (cervical, oral, etc.).
Most infections are asymptomatic and cleared by the immune system.
Prevention: Vaccination (Gardasil, Cervarix), Pap smears for women.
Human Immunodeficiency Virus (HIV)
Attacks CD4+ T cells, leading to acquired immunodeficiency syndrome (AIDS).
Transmitted via blood, sexual contact, or from mother to child.
No cure, but antiretroviral therapy (ART) controls infection and prolongs life.
Prevention and Risk Reduction
Abstinence and mutual monogamy between uninfected partners are the most effective prevention strategies.
Consistent and correct use of barrier contraception (condoms) reduces risk but does not eliminate it.
HPV vaccination and regular STI testing are recommended for sexually active individuals.
Prompt diagnosis and treatment prevent complications and further transmission.
Summary Table: Major Urinary and Reproductive Infections
Infection | Agent | Symptoms | Complications | Treatment |
|---|---|---|---|---|
UTI | UPEC, S. saprophyticus | Dysuria, urgency, pain | Pyelonephritis, renal failure | Antibiotics |
Chlamydia | C. trachomatis | Often asymptomatic, discharge, pain | PID, infertility, neonatal infection | Antibiotics |
Gonorrhea | N. gonorrhoeae | Often asymptomatic, discharge, pain | PID, infertility, DGI, blindness | Antibiotics (resistance rising) |
Syphilis | T. pallidum | Chancre, rash, systemic symptoms | Neurologic, cardiac, death | Antibiotics (early) |
Trichomoniasis | T. vaginalis | Discharge, itching, burning | Pregnancy complications | Antimicrobials |
HSV | HSV-1, HSV-2 | Painful blisters, ulcers | Recurrent outbreaks | Antivirals (not curative) |
HPV | HPV types 6, 11, 16, 18 | Warts, often asymptomatic | Cancer | Vaccine, screening |
HIV | HIV-1, HIV-2 | Immunodeficiency | AIDS, opportunistic infections | ART |
Key Takeaways
Most urinary and reproductive system infections are preventable and treatable if detected early.
Asymptomatic infections are common; regular screening is essential for sexually active individuals.
Antibiotic resistance is a growing concern, especially for gonorrhea.
Vaccination (HPV) and safe sexual practices are critical for prevention.
