 Back
BackVaccines and Immune Disorders: Mechanisms, Risks, and Clinical Implications
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Vaccines and Immune Disorders
Overview of Vaccine-Immune System Interactions
Vaccines are designed to safely stimulate the immune system to recognize and combat infectious agents. However, their interaction with the immune system—especially in individuals with immune disorders—can be complex. While vaccines are overwhelmingly safe, rare cases of immune-mediated adverse events have been documented, and their mechanisms are of significant interest in microbiology and immunology.
Autoimmune disorders are not commonly caused by vaccines, as shown by large-scale epidemiological studies.
Rare but confirmed associations exist between certain vaccines and specific immune-mediated conditions, but these are statistically very uncommon.
The risk of immune complications from natural infection is almost always higher than from vaccination.
Vaccine-Associated Immune-Mediated Conditions
Guillain-Barré Syndrome (GBS) and Influenza Vaccine
Guillain-Barré Syndrome (GBS) is a rare autoimmune neuropathy where the immune system attacks peripheral nerves, leading to muscle weakness and paralysis.
Risk after vaccination: 1–2 additional cases per million flu vaccine doses.
Historical context: The 1976 swine flu vaccine was associated with a higher risk (1 per 100,000), but current vaccines do not show this elevated risk.
Infection risk: Influenza infection itself is a much stronger trigger for GBS (17 cases per million infections).

Immune Thrombocytopenia (ITP) and MMR Vaccine
Immune thrombocytopenia (ITP) is a condition where the immune system destroys platelets, leading to bleeding symptoms such as petechiae and purpura.
Risk after MMR vaccine: About 1 case per 25,000–40,000 doses, most common in children aged 12–15 months.
Clinical course: Usually mild and self-limiting; 90% recover within six months.
Infection risk: Natural measles or rubella infections pose a much higher risk of ITP (up to 1 per 3,000).

Biological Mechanisms of Vaccine-Associated Autoimmunity
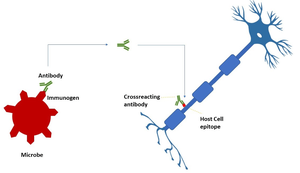
Molecular Mimicry (Cross-Reactivity)
Molecular mimicry occurs when a vaccine antigen closely resembles a human protein, causing the immune system to attack both the pathogen and self-tissues.
Example: Influenza vaccine components may mimic gangliosides on peripheral nerves, contributing to GBS.
Bystander Activation
In this mechanism, a strong immune response (often from infection or vaccination) creates an inflammatory environment that activates dormant autoreactive immune cells, leading to collateral tissue damage.
Epitope Spreading
Initial tissue damage from an immune response can release hidden self-antigens, broadening the autoimmune attack as the immune system targets these newly exposed proteins.
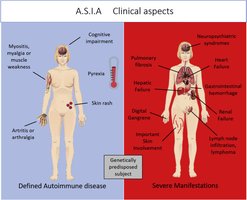
Adjuvant Effects (ASIA Syndrome)
Some vaccines contain adjuvants (e.g., aluminum salts) to enhance immune responses. In genetically susceptible individuals, these can cause prolonged inflammation, potentially leading to Autoimmune/Inflammatory Syndrome Induced by Adjuvants (ASIA).
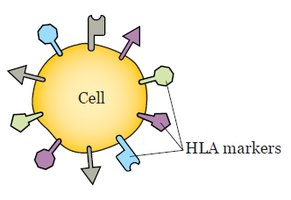
Genetic Predisposition
Genetic factors, especially certain Human Leukocyte Antigen (HLA) variants, influence susceptibility to vaccine-induced autoimmunity by affecting how antigens are presented to the immune system.
Vaccine Technology and Autoimmune Risk
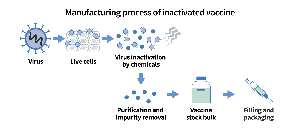
Traditional Inactivated Vaccines
Inactivated vaccines use whole, killed pathogens, exposing the immune system to a wide array of antigens. This increases the theoretical risk of molecular mimicry but is generally safe in practice.
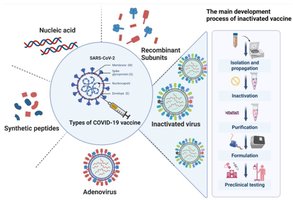
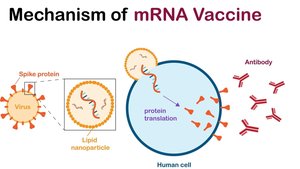
mRNA Vaccines
mRNA vaccines deliver genetic instructions for cells to produce a single pathogen protein (e.g., spike protein), reducing the number of potential mimics. The mRNA and lipid nanoparticles act as built-in adjuvants, stimulating innate immune sensors.
Adjuvants vs. Inbuilt Stimulation
Inactivated vaccines: Use chemical adjuvants to enhance immune response, which can rarely contribute to ASIA syndrome.
mRNA vaccines: Rely on the mRNA and lipid nanoparticles for immune stimulation, which can occasionally trigger bystander activation.
Immune Response Intensity
mRNA vaccines: Induce strong cellular (T-cell) responses, which may cause temporary flares in autoimmune conditions.
Inactivated vaccines: Induce milder, antibody-focused responses, often requiring more frequent boosters.
Vaccination in Individuals with Immune Disorders
Safety of Non-Live Vaccines
Inactivated (non-live) vaccines are generally safe and recommended for people with autoimmune diseases, as they do not replicate in the body.
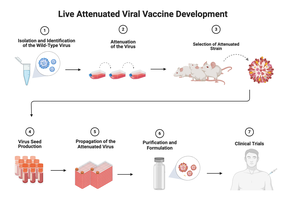
Caution with Live Vaccines
Live-attenuated vaccines are typically avoided in immunocompromised individuals due to the risk of causing disease.
Risk of Disease Flares
Vaccines can rarely trigger temporary flares in autoimmune diseases such as Lupus (SLE) or Rheumatoid Arthritis, but the benefits of vaccination outweigh these risks.
Mechanisms of Vaccine-Induced Flares in Lupus (SLE)
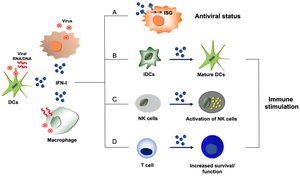
Biological Triggers
Type I Interferon (IFN-I) Induction: mRNA vaccines strongly stimulate IFN-I, which is central to SLE pathogenesis and can worsen symptoms.
Toll-Like Receptor (TLR) Activation: mRNA acts as a ligand for TLR-7, leading to exaggerated inflammation in SLE patients.
Molecular Mimicry: The SARS-CoV-2 spike protein shares short sequences with human proteins, but these similarities are usually too minor to cause autoimmunity.
Clinical and Individual Risk Factors
Active disease at vaccination: Higher SLEDAI scores or elevated anti-dsDNA antibodies increase flare risk.
Previous organ involvement: History of kidney or skin involvement increases risk after subsequent vaccine doses.
Repeated exposure: Flares are more common after second or third vaccine doses due to immune memory.
Summary Table: Vaccine-Associated Autoimmune Risks
Vaccine | Associated Condition | Estimated Risk | Risk from Infection |
|---|---|---|---|
Influenza | Guillain-Barré Syndrome | 1–2/million doses | 17/million infections |
MMR | Immune Thrombocytopenia | 1/25,000–40,000 doses | 1/3,000 (rubella) |
Key Takeaways
Vaccine-induced autoimmune disorders are extremely rare compared to the risks posed by natural infections.
Mechanisms include molecular mimicry, bystander activation, epitope spreading, and adjuvant effects, often requiring genetic predisposition.
Both traditional and mRNA vaccines are safe for most people, including those with immune disorders, though monitoring for flares is important.
Major medical organizations recommend vaccination for people with autoimmune diseases, as the benefits far outweigh the risks.
