 Back
BackVaricella Zoster Virus (VZV): Biology, Pathogenesis, Clinical Features, and Prevention
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Varicella Zoster Virus (VZV)
Basic Biology
The Varicella Zoster Virus (VZV) is a member of the Herpesviridae family and is known as Human herpesvirus 3 (HHV-3). It is a large, linear, double-stranded DNA virus with an envelope. Humans are the only natural host for VZV.
Family: Herpesviridae
Genome: Linear dsDNA
Envelope: Present
Host: Humans only
Transmission
VZV is highly contagious and spreads primarily through respiratory secretions and direct contact with fluid from skin lesions.
Respiratory route: Inhalation of droplets from mucus and saliva
Direct contact: Exposure to fluid from vesicular lesions
Groups at Increased Risk
Severe Primary Varicella (Chickenpox)
Certain populations are at higher risk for severe disease:
Infants under 1 year old
Pregnant women (especially early pregnancy; risk of congenital varicella syndrome)
Adults (more severe than in children)
Immunocompromised individuals (e.g., cancer, HIV, organ transplantation)
Risk Factors for Reactivation (Herpes Zoster/Shingles)
Older age (especially over 50)
Immunosuppression (HIV, malignancy, immunosuppressive drugs)
Stress, illness, physical trauma
Chronic medical conditions (diabetes, renal disease, lung disease)
Epidemiology
Chickenpox
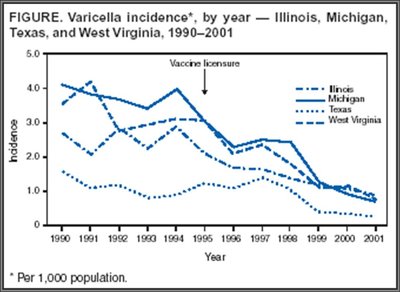
Chickenpox is highly contagious and most common in children aged 5–10 years. Vaccination has significantly reduced incidence in the U.S.
Incidence: Most common in children
Vaccine impact: Decreased cases post-vaccine introduction
Shingles
Occurs in about 5/1000 population
Immunosuppression increases risk
Clinical Presentation
Primary Infection: Chickenpox (Varicella)
Chickenpox typically presents after an incubation period of 10–21 days. Adults may experience a prodrome of fever, malaise, and headache. The hallmark is a vesicular rash appearing in crops, with lesions at different stages simultaneously.
Prodrome: Fever, malaise, loss of appetite, headache, fatigue
Rash: Begins on chest, back, and face, then spreads; lesions appear in crops and are at different stages
Other symptoms: Itching, low-grade fever
Complications: Secondary bacterial infections, pneumonia, encephalitis, congenital varicella syndrome


Reactivation: Shingles (Herpes Zoster)
Shingles presents with pain, burning, or tingling in a dermatomal distribution, followed by a unilateral vesicular rash. Pain can persist after rash resolution (postherpetic neuralgia).
Prodrome: Pain, burning, tingling, hypersensitivity
Rash: Red maculopapular rash evolving into vesicles and pustules; typically unilateral and restricted to one dermatome
Pain: Moderate to severe nerve pain, may persist as postherpetic neuralgia
Complications: Postherpetic neuralgia, ophthalmic zoster, secondary bacterial infections, disseminated zoster

Pathogenesis
Chickenpox (Primary Varicella Infection)
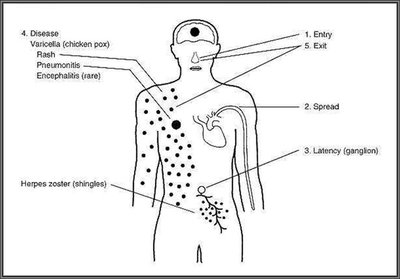
VZV enters via the respiratory tract, replicates in mucosa and lymph nodes, then spreads via viremia to the reticuloendothelial system and skin. The virus establishes latency in sensory ganglia after resolution.
Entry: Respiratory tract
Replication: Nasopharyngeal mucosa, lymph nodes
Primary viremia: Spread to liver, spleen, lymph nodes
Secondary viremia: Spread to skin and mucous membranes
Rash formation: Infection of epidermal cells, vesicular rash
Latency: Virus travels to dorsal root/cranial nerve ganglia
Shingles (Herpes Zoster Reactivation)
Years after primary infection, latent VZV reactivates in sensory ganglia due to weakened immunity. The virus travels down sensory nerves, causing localized inflammation and a dermatomal rash.
Reactivation: Latent virus reactivates in ganglia
Spread: Virus travels down sensory axons to skin
Rash: Dermatomal vesicular rash
Pain: Neuropathic pain from nerve inflammation
Diagnosis
Diagnostic Tests
Diagnosis is usually clinical, but laboratory tests can confirm VZV infection.
Rash examination
Blood test
Viral culture
Direct fluorescent antibody test

Treatment
Chickenpox
Usually no treatment required
Antihistamines for itching
Shingles
Antiviral medications: Acyclovir, Famciclovir
NSAIDs for pain
Capsaicin topical cream for postherpetic neuralgia
Prevention
Varicella (Chickenpox) Vaccine
The live attenuated vaccine (Varivax) is highly effective, preventing about 98% of moderate to severe disease.

Herpes Zoster (Shingles) Vaccine
Recombinant zoster vaccine (RZV, Shingrix) is preferred in the U.S.
Reduces risk of shingles and postherpetic neuralgia by >90%
Quiz Questions
Hallmark Sign of Chickenpox
Correct answer: Vesicular lesions appearing in crops at different stages
Pathogenesis of Shingles in Immunocompromised Patient
Correct answer: Latent VZV reactivated in sensory ganglia and spread down nerve axons
Prevention Plan for Nursing Home
Correct answer: Provide recombinant zoster vaccine to residents ≥50 years and varicella vaccine to non-immune staff
