 Back
BackDisorders in Immunity: Hypersensitivities, Autoimmunity, and Immunodeficiencies
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Disorders in Immunity
Overview of Immune System Disorders
The immune system is essential for defending the body against pathogens, but abnormal immune responses can lead to disease. Immunopathology is the study of diseases caused by overreactivity (hypersensitivity) or underreactivity (immunodeficiency) of the immune system. These disorders include allergies, autoimmunity, and immunodeficiencies.
Hypersensitivity: Overreactivity of the immune system, including allergies and autoimmunity.
Hyposensitivity (Immunodeficiency): Underreactivity or failure of the immune system, leading to increased susceptibility to infections.

Hypersensitivity Reactions
Types of Hypersensitivity
Hypersensitivity reactions are classified into four types based on their mechanisms and clinical manifestations:
Type I (Immediate): IgE-mediated reactions, such as allergies and anaphylaxis.
Type II (Antibody-mediated): IgG and IgM antibodies target cells, leading to cell lysis (e.g., blood transfusion reactions).
Type III (Immune Complex-mediated): Immune complexes deposit in tissues, causing inflammation (e.g., rheumatoid arthritis).
Type IV (Cell-mediated): T-cell mediated, delayed reactions (e.g., contact dermatitis, graft rejection).
Type I Hypersensitivity: Allergy and Anaphylaxis
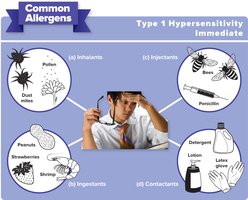
Type I hypersensitivity involves an exaggerated immune response to harmless antigens (allergens), resulting in inflammation. Common allergens include inhalants, ingestants, injectants, and contactants.
Allergens: Substances that trigger allergic reactions in sensitive individuals.
Atopy: Chronic local allergy (e.g., hay fever, asthma).
Anaphylaxis: Severe, systemic allergic reaction that can be life-threatening.
Cellular Mechanisms of Type I Allergy
The allergic response involves two main phases: sensitization and subsequent exposure. During sensitization, B cells produce IgE antibodies that bind to mast cells. Upon re-exposure, allergens cross-link IgE on mast cells, triggering degranulation and release of inflammatory mediators.
Sensitization: Initial exposure leads to IgE production and binding to mast cells.
Degranulation: Re-exposure causes mast cells to release histamine and other mediators, leading to symptoms.

Effects of Allergic Mediators
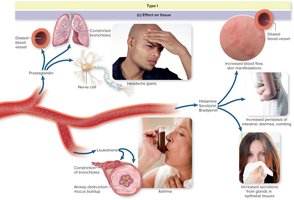
Allergic mediators such as histamine, leukotrienes, prostaglandins, and bradykinin cause various symptoms by acting on target tissues:
Histamine: Vasodilation, increased vascular permeability, bronchoconstriction, and itching.
Leukotrienes: Prolonged bronchospasm and mucus secretion.
Prostaglandins: Vasodilation, pain, and bronchoconstriction.
Bradykinin: Smooth muscle contraction and increased mucus secretion.
Clinical Manifestations of Type I Hypersensitivity
Hay Fever (Allergic Rhinitis): Nasal congestion, sneezing, itchy eyes, and mild bronchoconstriction.
Asthma: Episodes of impaired breathing due to bronchoconstriction, often triggered by inhaled allergens.
Atopic Dermatitis (Eczema): Itchy, inflamed skin lesions, often beginning in infancy.
Food Allergy: Gastrointestinal symptoms (vomiting, diarrhea, abdominal pain) and possible systemic reactions.
Drug Allergy: Reactions to medications, ranging from mild rash to anaphylaxis.


Diagnosis and Treatment of Allergies
Allergies can be diagnosed using in vitro (blood tests) and in vivo (skin tests) methods. Treatment involves blocking allergic pathways, avoiding allergens, and desensitization.
In vitro tests: Measure IgE levels, tryptase, and histamine release.
In vivo tests: Skin prick tests to identify specific allergens.
Treatment: Antihistamines, corticosteroids, cromolyn, and desensitization therapy.


Type II Hypersensitivity: Antibody-Mediated Reactions
Mechanism and Clinical Importance
Type II hypersensitivity involves IgG and IgM antibodies targeting antigens on cell surfaces, leading to cell lysis via complement activation. Examples include transfusion reactions and hemolytic disease of the newborn (HDN).
Alloantigens: Antigens that differ within a species, such as blood group antigens.
Rh factor: An antigen on red blood cells; incompatibility can cause HDN.
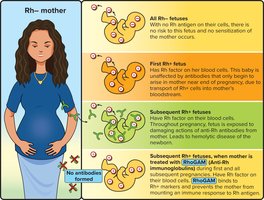
Hemolytic Disease of the Newborn (HDN)
HDN occurs when an Rh-negative mother is sensitized to Rh-positive fetal blood cells, leading to the production of anti-Rh antibodies that attack fetal red blood cells in subsequent pregnancies.
Prevention: RhoGAM antiserum is administered to Rh-negative mothers to prevent sensitization.

Type III Hypersensitivity: Immune Complex Reactions
Mechanism and Examples
Type III hypersensitivity involves the formation of antigen-antibody complexes that deposit in tissues, activating complement and causing inflammation. Unlike type II, the antigens are soluble and not cell-bound.
Example: Acute post-streptococcal glomerulonephritis (APSGN), where immune complexes deposit in the kidneys, causing damage.
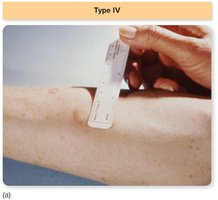
Type IV Hypersensitivity: Cell-Mediated (Delayed) Reactions
Mechanism and Clinical Examples
Type IV hypersensitivity is mediated by T cells and does not involve antibodies. Symptoms develop 1–3 days after exposure. Examples include the tuberculin skin test and contact dermatitis (e.g., poison ivy).
Host vs. Graft: Recipient T cells attack transplanted tissue.
Graft vs. Host: Donor immune cells attack recipient tissues (e.g., after bone marrow transplant).


Classes of Grafts
Autograft: From one site to another on the same individual.
Isograft: Between genetically identical individuals (e.g., identical twins).
Allograft: Between genetically different individuals of the same species.
Xenograft: Between individuals of different species.

Autoimmunity
Mechanisms and Examples
Autoimmune diseases occur when the immune system attacks self-antigens. They may be systemic or organ-specific and are influenced by genetic, environmental, and infectious factors.
Systemic lupus erythematosus (SLE): Autoantibodies against multiple organs and tissues.
Rheumatoid arthritis: Immune complexes in joints cause chronic inflammation.
Graves’ disease: Autoantibodies stimulate the thyroid gland, causing hyperthyroidism.
Type I diabetes: Cytotoxic T cells destroy pancreatic beta cells.
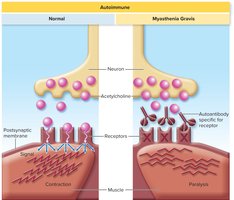
Myasthenia gravis: Autoantibodies block acetylcholine receptors at neuromuscular junctions, leading to muscle weakness.
Multiple sclerosis: T cells and autoantibodies damage myelin in the central nervous system.

Immunodeficiency Diseases
Primary and Secondary Immunodeficiencies
Immunodeficiencies are characterized by weakened immune responses, leading to recurrent infections. They may be primary (congenital, genetic) or secondary (acquired after birth).
Primary immunodeficiencies: Genetic defects affecting B cells, T cells, or both (e.g., SCID, DiGeorge syndrome, agammaglobulinemia).
Secondary immunodeficiencies: Result from infections (e.g., AIDS), cancer, malnutrition, or immunosuppressive therapy.

Summary Table: Types of Immune Disorders
Disorder | Mechanism | Examples |
|---|---|---|
Type I Hypersensitivity | IgE-mediated, mast cell degranulation | Hay fever, asthma, anaphylaxis |
Type II Hypersensitivity | IgG/IgM-mediated cell lysis | Transfusion reaction, HDN |
Type III Hypersensitivity | Immune complex deposition | Serum sickness, APSGN |
Type IV Hypersensitivity | T-cell mediated, delayed | Contact dermatitis, graft rejection |
Autoimmunity | Immune response to self-antigens | Lupus, rheumatoid arthritis, type I diabetes |
Immunodeficiency | Deficient immune response | SCID, AIDS |
