 Back
BackGram-Positive Cocci of Medical Importance: Staphylococcus, Streptococcus, and Enterococcus
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Gram-Positive Cocci of Medical Importance
Overview
Gram-positive cocci are a significant group of bacteria in clinical microbiology, including common normal flora and important human pathogens. They are characterized by their spherical shape, Gram-positive cell wall, and lack of endospore formation. Many infections caused by these organisms are pyogenic, meaning they stimulate pus formation.
Common genera: Staphylococcus, Streptococcus, Enterococcus
Clinical importance: Range from mild skin infections to life-threatening systemic diseases
Notable feature: Many are part of the normal human flora but can become opportunistic pathogens
Staphylococcus
General Characteristics
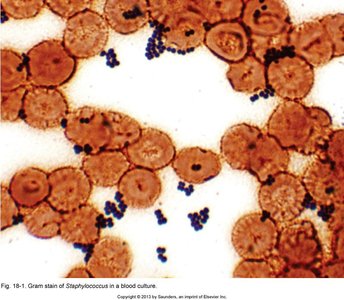
Staphylococcus species are Gram-positive cocci that typically form clusters. They are catalase positive, non-motile, and may possess capsules. These bacteria are common inhabitants of the skin and mucous membranes.
Arrangement: Clusters (staphyle)
Catalase test: Positive (distinguishes from Streptococcus)
Flagella: Absent
Capsules: May be present
Species: Over 45 identified
Staphylococcus aureus
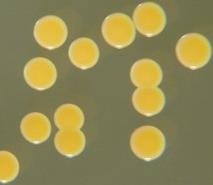
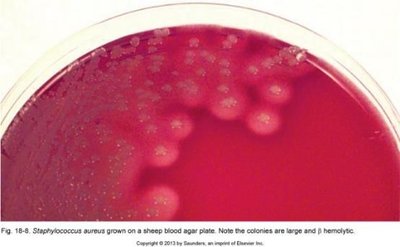
Staphylococcus aureus is the most clinically significant species, known for its golden-yellow colonies and numerous virulence factors. It is a facultative anaerobe and can withstand harsh environmental conditions.
Colony morphology: Large, round, opaque, golden yellow on certain media
Growth temperature: Optimum at 37°C (mesophile)
Resistance: Withstands high salt, extremes in pH, and high temperatures
Virulence factors: Capsule/slime layer, Protein A, lipases, coagulase, cytolysins, exfoliative toxins, enterotoxins, toxic shock syndrome toxin

Virulence Factors
Glycocalyx: Capsule or slime layer for evasion of host defenses
Protein A: Binds Fc region of IgG, interfering with opsonization
Coagulase: Promotes clot formation, protecting bacteria from immune cells
Cytolysins: Damage cell membranes (e.g., alpha, beta, gamma, delta toxins, PV leukocidin)
Exfoliative toxins: Proteases that damage skin proteins
Enterotoxins & Toxic Shock Syndrome Toxin: Superantigens causing systemic effects
Epidemiology and Pathogenesis
Reservoir: Anterior nares (nostrils) of healthy adults (carriage rate ~60%)
Transmission: Fomites, direct contact
Predisposing factors: Poor hygiene, injury, diabetes, immunodeficiency
Antibiotic resistance: >95% produce beta-lactamases; MRSA (mecA gene), VISA/VRSA emerging
Staphylococcal Diseases
Localized Cutaneous Infections
Folliculitis: Inflammation of hair follicle (stye if on eyelid)
Furuncle: Boil; abscess formation
Carbuncle: Larger, deeper lesion formed by cluster of furuncles
Impetigo: Pus-filled lesions on reddened base
Mastitis: Infection of breast during lactation



Systemic Infections
Osteomyelitis: Bone infection, especially in children and adults (vertebrae)
Endocarditis: Infection of heart valves
Pneumonia, septic arthritis
Treatment: Long-term antibiotics (e.g., clindamycin, TMP-SMX)
Toxigenic Diseases
Food intoxication: Ingestion of heat-stable enterotoxins; rapid onset of GI symptoms
Staphylococcal scalded skin syndrome: Exfoliative toxin causes skin desquamation
Toxic shock syndrome: Superantigen-mediated toxemia, shock, organ failure


Other Staphylococci
S. epidermidis: Normal flora; can cause endocarditis, bacteremia, UTI
S. saprophyticus: Second most common cause of UTIs in young women
S. lugdunensis, S. hominis, S. haemolyticus, S. capitis: Opportunistic infections
Identification of Staphylococcus
Sample types: Pus, tissue exudates, sputum, urine, blood
PCR: For specific DNA or resistance genes
Cultivation: Blood agar, mannitol salt agar
Catalase test: Positive for Staphylococcus
Coagulase test: Positive for S. aureus
Streptococcus
General Characteristics
Streptococcus species are Gram-positive cocci that form chains. They are catalase negative, non-motile, and often require enriched media for growth. Many are sensitive to drying and disinfectants.
Arrangement: Chains
Catalase test: Negative (distinguishes from Staphylococcus)
Capsules/slime layers: May be present
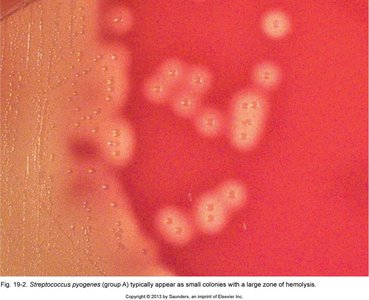
Colony morphology: Small, non-pigmented
Classification of Streptococcus
Hemolysis on blood agar:
Alpha (α): Partial (greenish, "bruising")
Beta (β): Complete (clear zone)
Gamma (γ): None
Lancefield grouping: Based on cell wall antigens (Groups A, B, C, etc.)

Streptococcus pyogenes (Group A Streptococcus, GAS)
Hemolysis: Beta-hemolytic
Habitat: Throat, nasopharynx, occasionally skin
Strict parasite: Humans only reservoir
Virulence Factors
C-carbohydrates: Protect from lysozyme
Fimbriae: Adherence to surfaces
M-protein: Resists phagocytosis, blocks complement
Hyaluronic acid capsule: Mimics host tissue
C5a protease (ScpA): Inactivates complement components
Streptolysins (O, S): Damage cell membranes
Streptococcal pyrogenic exotoxins (SPE): Induce fever, rash
Streptokinase: Digests clots
Hyaluronidase: Breaks down connective tissue
DNAse: Degrades DNA in neutrophil extracellular traps (NETs)
Epidemiology and Pathogenesis
Transmission: Contact, droplets, food, fomites
Portal of entry: Skin or pharynx
Population affected: Mostly children
Carriers: Up to 15% inapparent carriers
Clinical Diseases Caused by Streptococcus pyogenes
Skin Infections
Impetigo: Contagious, crusted lesions
Erysipelas: More invasive, well-demarcated borders
Cellulitis: Deeper, less defined borders
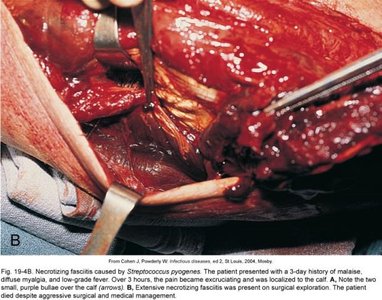
Necrotizing fasciitis: "Flesh-eating bacteria"; rapid tissue destruction, high mortality



Throat Infections
Streptococcal pharyngitis (strep throat): Sore throat, fever, red pharynx

Systemic Diseases
Scarlet fever: SPE toxin causes fever, sandpapery rash
Septicemia, pneumonia, toxic shock syndrome

Sequelae (Post-infection Complications)
Rheumatic fever: Autoimmune reaction after pharyngitis; affects heart, joints, CNS
Acute glomerulonephritis: Immune complex deposition in kidneys; can lead to chronic renal failure
Group B Streptococcus: Streptococcus agalactiae
Hemolysis: Beta-hemolytic
Habitat: Vagina, throat, large intestine (25% carriage)
Clinical importance: Severe neonatal infections (pneumonia, sepsis, meningitis)
Prevention: Screening pregnant women (weeks 35-37), intrapartum antibiotics
Identification of Beta-Hemolytic Streptococcus spp.
Rapid diagnostic tests: Monoclonal antibodies for Lancefield groups
Cultural tests: Bacitracin sensitivity (GAS +), CAMP test (GBS +)

Treatment and Prevention
Groups A and B: Penicillin (some reduced sensitivity emerging)
Alternatives: Used for penicillin-allergic patients
Long-term prophylaxis: For history of rheumatic fever or recurrent strep throat
Alpha-Hemolytic Streptococci: Viridans Group
Species: S. mutans, S. oralis, S. salivarius, others
Habitat: Oral cavity, nasopharynx, genital tract, skin
Diseases: Dental caries, tooth abscesses, subacute endocarditis (especially in heart disease)
Streptococcus pneumoniae (Pneumococcus)
Shape: Lancet-shaped diplococci
Hemolysis: Alpha-hemolytic
Virulence factor: Capsule (90 types)
Diseases: Pneumonia, meningitis, otitis media
Diagnosis: Gram stain, Quellung reaction, optochin sensitivity, bile solubility
Prevention: Vaccines (23-valent polysaccharide, 13-valent conjugate)
Enterococci
General Characteristics
Lancefield Group D: Enterococcus faecalis, E. faecium, E. durans
Habitat: Normal flora of large intestine
Diseases: Opportunistic UTIs, wound, and skin infections (especially in debilitated patients)
Antibiotic resistance: Increasing, second most common nosocomial infection after Staphylococci
Hemolysis: Can be alpha, beta, or gamma
Identification of Enterococci
Colony morphology: Usually large colonies
Bile esculin test: Positive for Enterococcus
Optochin resistance: Enterococcus resistant
PYR test: Production of L-pyrrolidonyl arylamidase (cherry red positive)
