 Back
BackMicrobial Diseases of the Urinary and Reproductive Systems: Study Notes
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Microbial Diseases of the Urinary and Reproductive Systems
Overview
This chapter explores the major microbial diseases affecting the urinary and reproductive systems, focusing on bacterial, viral, and parasitic infections. It covers the etiology, pathogenesis, clinical manifestations, diagnosis, treatment, and prevention of these diseases, with emphasis on sexually transmitted infections (STIs) and urinary tract infections (UTIs).
Urinary Tract Infections (UTIs)
Types and Etiology
Urethritis: Inflammation of the urethra.
Cystitis: Inflammation of the bladder, often due to Escherichia coli (E. coli) and other Gram-negative bacteria.
Pyelonephritis: Infection of the kidneys, which may develop from untreated cystitis. Scar tissue formation can impair kidney function and become life-threatening.
Most UTIs are caused by opportunistic pathogens from fecal contamination, especially normal microbiota of the small intestine. Nosocomial infections can occur after catheterization, with Pseudomonas aeruginosa as a common agent.
Treatment: Broad-spectrum antibiotics; kidney dialysis may be required for severe pyelonephritis.
Sexually Transmitted Infections (STIs)
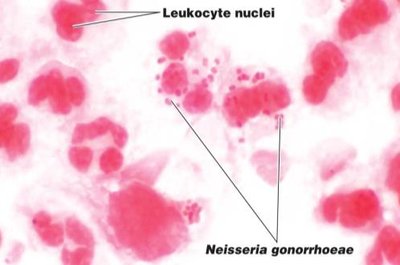
Gonorrhea (Neisseria gonorrhoeae)
Gonorrhea is a common STI caused by the Gram-negative diplococcus Neisseria gonorrhoeae. It infects mucous membranes of the reproductive tract, and can also affect the pharynx and rectum.
Males: Usually symptomatic within one week; symptoms include painful urination and purulent discharge from the urethra.
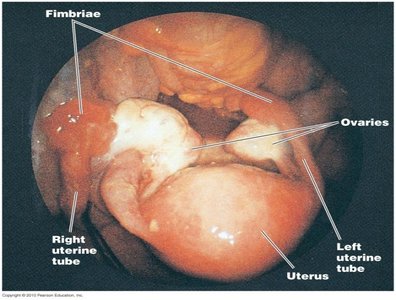
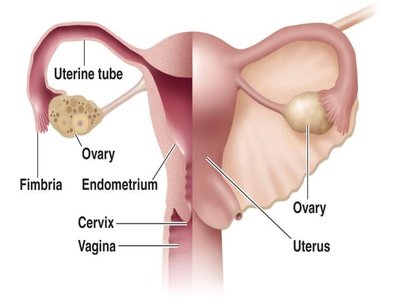
Females: Often asymptomatic in early stages; can progress to pelvic inflammatory disease (PID), affecting the ovaries, fallopian tubes, and uterus, potentially leading to sterility.
Complications: Untreated infections may become systemic, affecting joints, heart, and meninges. Can cause gonorrheal ophthalmia in newborns.
Treatment: Antibiotics (resistance is common); prevention includes condom use and prophylactic eye drops for newborns.

Chlamydial Infections (Chlamydia trachomatis)
Chlamydia is the most common STI in North America, caused by the intracellular parasite Chlamydia trachomatis. It infects the epithelial cells of the urogenital tract.
Males: Symptoms are similar to gonorrhea but milder.
Females: Often asymptomatic; untreated infections can lead to PID.
Treatment: Broad-spectrum antibiotics; cell wall-active agents are ineffective because Chlamydia lacks a peptidoglycan cell wall.
Syphilis (Treponema pallidum)
Syphilis is a chronic STI caused by the spirochete Treponema pallidum. It is transmitted through direct contact with infectious lesions and progresses through three stages:
Primary Stage: Occurs ~3 weeks post-exposure; characterized by a painless chancre at the site of infection (may be unnoticed if internal).
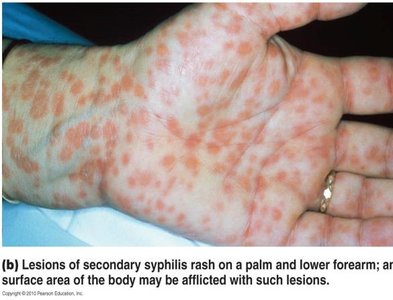
Secondary Stage: Develops several weeks later; widespread skin rashes and mucous membrane lesions, highly infectious. Non-sexual transmission is possible.
Tertiary Stage: Occurs years after latency; not contagious or treatable. Manifestations include gummatous syphilis (rubbery lesions), cardiovascular syphilis (aortic weakening), and neurosyphilis (CNS involvement: dementia, seizures, paralysis, death).
Treatment: Antibiotics are effective only in the first and second stages.


Viral STIs
Genital Herpes (Herpes Simplex Virus 2, HSV-2)
Genital herpes is primarily caused by HSV-2, though HSV-1 can also be involved. The infection is characterized by painful vesicular lesions and can enter a latent phase in nerve cells.
Symptoms: Burning, irritation, painful urination, vesicles containing infectious fluid.
Latency: Virus remains dormant in nerve cells; can reactivate due to stress, illness, menstruation, or UV exposure.
Transmission: Can occur even when lesions are not visible; condoms may not fully protect.
Treatment: Acyclovir inhibits viral replication but is only effective against active lesions.

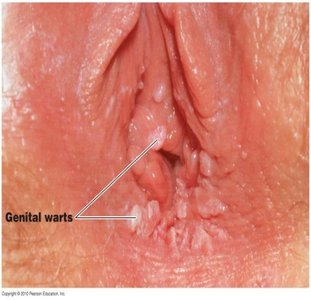
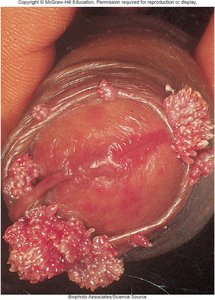
Genital Warts (Human Papillomavirus, HPV)
HPV is a group of viruses that infect skin and mucous membranes, causing genital warts and increasing the risk of cervical and other cancers.
Transmission: Direct contact with infected lesions; condoms may not fully prevent transmission.
Complications: High-risk HPV types are associated with cervical, oral, anal, and penile cancers.
Prevention: Vaccines are available and protect against the most oncogenic HPV types.
Human Immunodeficiency Virus (HIV) and AIDS
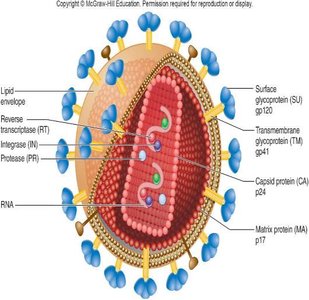
HIV Structure and Replication
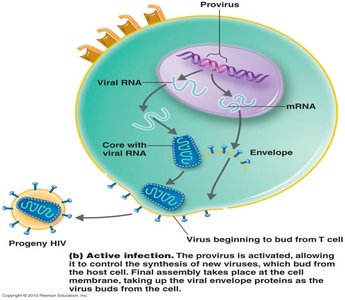
HIV is an enveloped retrovirus that infects CD4+ T cells. Its spikes enable attachment and penetration of host cells. The viral RNA is reverse transcribed and integrated into the host genome as a provirus, allowing for latency and immune evasion.
Active Infection: New viruses bud from the host cell membrane, acquiring their envelope.
Antigenic Variation: High mutation rate leads to frequent antigenic changes, complicating immune response and vaccine development.
HIV-1: Most common worldwide.
HIV-2: Found mainly in West Africa; slower disease progression.
Stages of HIV Infection
Category A (Early Stage): Often asymptomatic or mild flu-like symptoms; high TH cell count, low viral load.
Category B (Middle Stage): May be asymptomatic or present with persistent infections (e.g., yeast infections, shingles, diarrhea); TH cells decline, HIV resides in lymph nodes. This stage can last 10–20 years.
Category C (Late Stage/Clinical AIDS): Defined by a significant decrease in TH cells; persistent opportunistic infections (e.g., esophageal candidiasis, pneumonia, Kaposi’s sarcoma).
HIV Transmission
Blood: Needle sharing, occupational exposure; high viral load (1000–100,000 viruses/mL).
Semen/Vaginal Secretions: Unprotected sexual contact; lower viral load (10–50 viruses/mL).
Mother to Child: Transmission during pregnancy, birth, or breastfeeding.
Saliva: Very low risk; less than 1 virus/mL.
Survival: HIV survives ~1.5 days within cells outside the body, ~6 hours outside cells.
Summary Table: Major Microbial Diseases of the Urinary and Reproductive Systems
Disease | Pathogen | Symptoms | Treatment | Prevention |
|---|---|---|---|---|
UTIs | E. coli, P. aeruginosa | Dysuria, frequency, urgency, pyelonephritis | Broad-spectrum antibiotics | Hygiene, catheter care |
Gonorrhea | Neisseria gonorrhoeae | Urethral discharge, PID, systemic infection | Antibiotics (resistance common) | Condoms, eye drops for newborns |
Chlamydia | Chlamydia trachomatis | Mild or asymptomatic, PID | Broad-spectrum antibiotics | Condoms, screening |
Syphilis | Treponema pallidum | Chancre, rash, gummas, CNS symptoms | Antibiotics (early stages) | Condoms, screening |
Genital Herpes | HSV-2, HSV-1 | Painful vesicles, latency, recurrences | Acyclovir (active lesions) | Safe sex (partial protection) |
Genital Warts | HPV | Warts, cancer risk | Removal, vaccine | Vaccine, safe sex |
HIV/AIDS | HIV-1, HIV-2 | Immunodeficiency, opportunistic infections | Antiretroviral therapy | Safe sex, needle safety, screening |
