 Back
BackMicrobial Diseases of the Urinary and Reproductive Systems
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Structure and Function of the Urinary System
Overview of the Urinary System
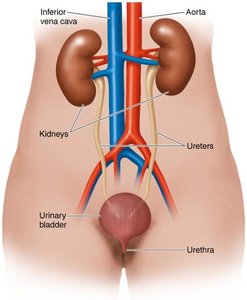
The urinary system is responsible for the removal of waste products from the bloodstream and the regulation of water and electrolyte balance. It consists of two kidneys, two ureters, one urinary bladder, and one urethra. Several anatomical and physiological features help prevent infection, including valves that prevent backflow to the kidneys, the acidity of urine, and mechanical flushing during urination.
Kidneys: Filter blood and produce urine.
Ureters: Transport urine from the kidneys to the bladder.
Urinary bladder: Stores urine until excretion.
Urethra: Conducts urine out of the body.
Infection prevention: Valves, urine acidity, and flushing action.
Structure and Function of the Genital Systems
Female Genital System
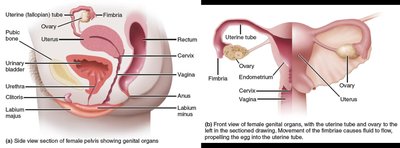
The female genital system includes two ovaries, two uterine (fallopian) tubes, the uterus (including the cervix), the vagina, and the external genitals (vulva). These organs are involved in reproduction, hormone production, and protection against pathogens.
Ovaries: Produce eggs and hormones.
Uterine tubes: Transport eggs from ovaries to uterus.
Uterus: Site of fetal development.
Vagina: Receives sperm and serves as the birth canal.
Vulva: External genitalia.
Male Genital System
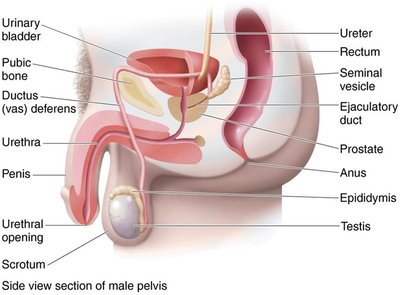
The male genital system consists of two testes, a system of ducts (epididymis, ductus (vas) deferens, ejaculatory duct, urethra), accessory glands, and the penis. These structures are essential for sperm production, maturation, and delivery.
Testes: Produce sperm and testosterone.
Epididymis: Sperm maturation and storage.
Vas deferens, ejaculatory duct, urethra: Transport sperm.
Accessory glands: Produce seminal fluid.
Penis: Delivers sperm to the female reproductive tract.
Normal Microbiota of the Urinary and Genital Systems
Microbial Flora
Normal urine is not sterile and contains a variety of microbes. The predominant microbes of the vagina are Lactobacilli, whose growth is promoted by estrogen. Other organisms include Streptococci species, anaerobes, some gram-negatives, and the yeast Candida albicans. In males, the urethra introduces bacteria into semen, with microbes such as Propionibacterium sp., Prevotella sp., and Lactobacillus sp. present in the seminal vesicles.
Bacterial Diseases of the Urinary System
Types of Infections
Bacterial infections of the urinary system include urethritis (inflammation of the urethra), cystitis (inflammation of the bladder), ureteritis (infection of the ureters), and pyelonephritis (inflammation of one or both kidneys). Over 7 million urinary tract infections (UTIs) occur annually, most commonly caused by Escherichia coli.
Cystitis: Commonly caused by E. coli and Staphylococcus saprophyticus. Symptoms include dysuria (painful urination) and pyuria (pus in urine). More common in women due to anatomical factors. Diagnosed by >1,000 CFUs/mL and a positive leukocyte esterase (LE) test. Treated with nitrofurantoin or a fluoroquinolone.
Pyelonephritis: 75% of cases caused by E. coli. Symptoms include fever and back/flank pain. Can lead to bacteremia and kidney scarring. Diagnosed by >100,000 CFUs/mL and a positive LE test. Treated with second or third generation cephalosporins.
Table: Common Bacterial Diseases of the Urinary System
Disease | Pathogen | Symptoms | Diagnosis | Treatment |
|---|---|---|---|---|
Cystitis | E. coli, Staphylococcus saprophyticus | Painful urination | >1,000 CFU/mL, +LE test | Nitrofurantoin |
Pyelonephritis | Primarily E. coli | Fever, back/flank pain | >100,000 CFU/mL, +LE test | Cephalosporin |
Leptospirosis | Leptospira interrogans | Headache, muscle aches, fever, possible kidney failure | Serological test | Doxycycline |
Diseases of the Genital Systems
Sexually Transmitted Infections (STIs)
STIs, formerly known as sexually transmitted diseases (STDs), are often asymptomatic, facilitating their spread. Over 30 types of infections exist, with 60 million new cases annually in the U.S., half among 15-24-year-olds. Most STIs can be prevented with condom use.
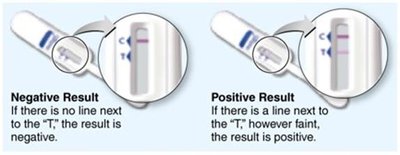
STI Home Test Kits
Home test kits allow individuals to collect samples and mail them to a lab for screening of chlamydia, gonorrhea, trichomoniasis, HIV, and urinary tract infections. Nucleic acid amplification tests (NAATs) are commonly used. Pros include increased diagnosis and access; cons include cost, privacy, and accuracy concerns.
Major Bacterial STIs
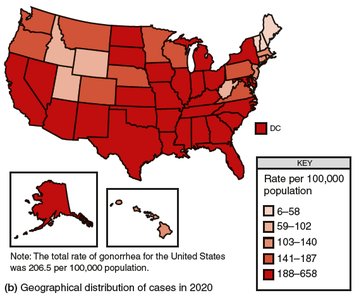
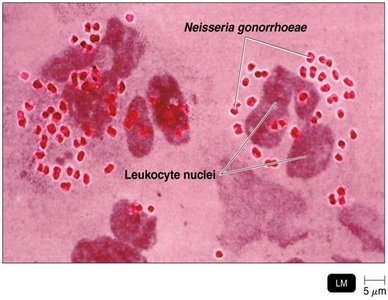
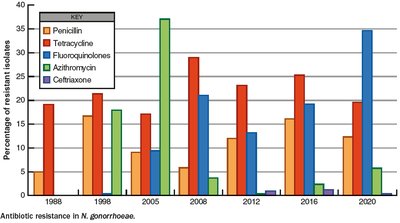
Gonorrhea
Gonorrhea is caused by Neisseria gonorrhoeae, a gram-negative diplococcus. The bacterium attaches to epithelial mucosa via fimbriae and invades spaces between columnar epithelial cells, causing inflammation and pus formation. It can infect the pharynx, eyes, rectum, urethra, cervix, and external genitalia.
Symptoms: Men experience painful urination and pus discharge; women may have mild symptoms but risk pelvic inflammatory disease (PID).
Complications: Untreated infections can lead to endocarditis, meningitis, arthritis, and ophthalmia neonatorum in infants.
Treatment: Ceftriaxone is the drug of choice.
Prevention: Erythromycin drops in neonates' eyes prevent ophthalmia neonatorum.

Nongonococcal Urethritis (NGU)
NGU refers to urethritis not caused by N. gonorrhoeae. The most common cause is Chlamydia trachomatis, followed by Mycoplasma genitalium and Ureaplasma urealyticum. Symptoms include painful urination and watery discharge, but many cases are asymptomatic. Complications in women include PID. Diagnosis is by NAATs; treatment is with azithromycin or doxycycline.
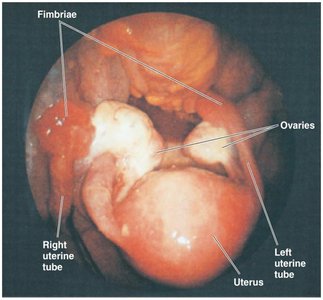
Pelvic Inflammatory Disease (PID)
PID is an extensive bacterial infection of the female pelvic organs, often polymicrobial (commonly N. gonorrhoeae and C. trachomatis). It can cause infertility and chronic pain. Salpingitis (infection of uterine tubes) is the most serious form, leading to scarring and ectopic pregnancy. Treatment involves doxycycline, ceftriaxone, and metronidazole.
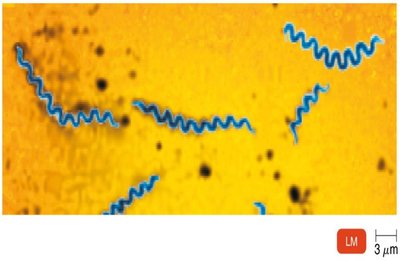
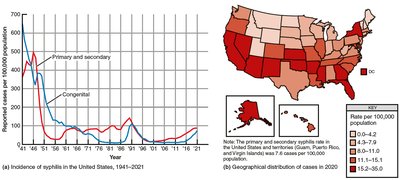
Syphilis
Syphilis is caused by Treponema pallidum, a gram-negative spirochete. It invades mucosa or skin breaks and enters the bloodstream, causing an inflammatory response. The disease progresses through several stages:
Primary: Chancre at infection site (painless, highly infectious).
Secondary: Skin and mucosal rashes, especially on palms and soles.
Latent: No symptoms.
Tertiary: Gummas, cardiovascular and neurological damage.
Congenital: Transmitted across placenta, causing fetal damage.

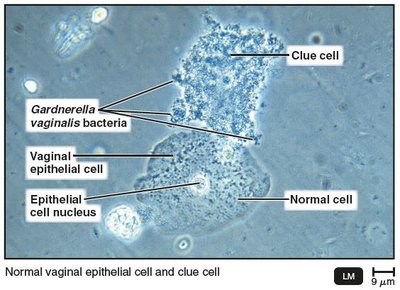
Bacterial Vaginosis
Bacterial vaginosis (BV) is caused by an imbalance of vaginal flora, with a decrease in protective Lactobacillus and overgrowth of anaerobic bacteria such as Gardnerella vaginalis. It is associated with a pH above 4.5, fishy odor, and frothy discharge. Clue cells (vaginal epithelial cells covered with bacteria) are diagnostic. Treated with metronidazole.
Major Viral and Fungal STIs
Genital Herpes
Genital herpes is caused by Herpes Simplex Virus 2 (HSV-2), and sometimes HSV-1. It presents as painful vesicles on the genitals and may recur due to latency in nerve cells. Diagnosis is by cell culture or PCR. There is no cure; management is with acyclovir, famciclovir, or valacyclovir.

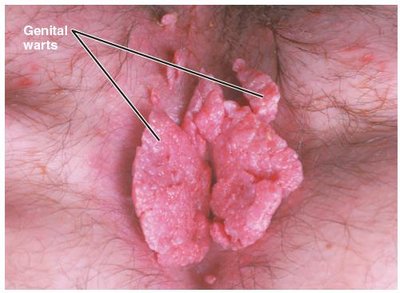
Genital Warts
Genital warts (condyloma acuminata) are caused by human papillomaviruses (HPV), with over 60 types. Types 6 and 11 cause visible warts; types 16 and 18 are associated with cervical cancer. Treated by removal, podofilox, or imiquimod; prevented by HPV vaccines.
Candidiasis
Candidiasis is caused by the fungus Candida albicans. It can affect the mouth (thrush), intestinal tract, and genitourinary tract. Overgrowth is often due to antibiotics, diabetes, or hormonal changes. Vulvovaginal candidiasis presents with a thick, yellow discharge. Diagnosis is by microscopy or culture; treated with clotrimazole or fluconazole.
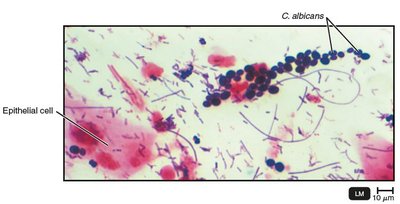
Table: Characteristics of Common Types of Vaginitis and Vaginosis
Disease | Pathogen | Discharge | Amount | Appearance | pH | Diagnosis | Treatment |
|---|---|---|---|---|---|---|---|
Bacterial Vaginosis | G. vaginalis, A. vaginae, Megasphaera | Fishy, gray-white, thin, frothy | Copious | Pink | >4.5 | Clue cells | Metronidazole |
Candidiasis | C. albicans | Yeasty, white, curdy | Varies | Dry, red | <4 | Microscopy | Clotrimazole, Miconazole |
Trichomoniasis | T. vaginalis | Foul, greenish-yellow, frothy | Copious | Tender, red | 5–6 | Microscopy, DNA probes | Metronidazole |
Acquired Immunodeficiency Syndrome (AIDS)
Origin and Structure of HIV
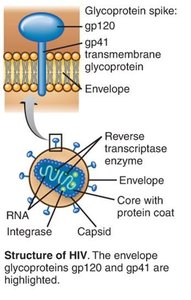
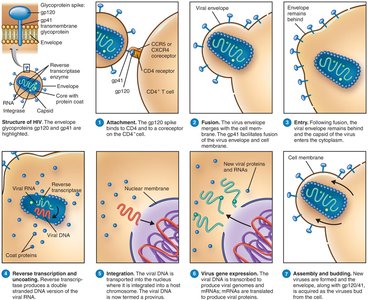
HIV is a retrovirus that crossed into humans from chimpanzees in Africa. It contains two identical +ssRNA molecules, reverse transcriptase, integrase, and a phospholipid envelope with gp120 glycoprotein spikes.
HIV Infection and Pathogenicity
HIV is picked up by dendritic cells and brought to lymphoid organs, where it infects CD4+ T cells. The gp120 spike binds to CD4 and a coreceptor (CCR5 or CXCR4), allowing viral entry. Inside the cell, viral RNA is reverse transcribed to DNA and integrated into the host genome. HIV evades the immune system by latency, cell-cell fusion, and rapid mutation.
Stages of HIV Infection
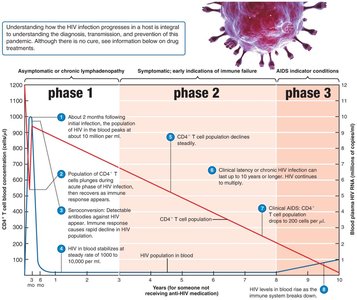
Phase 1: Asymptomatic or lymphadenopathy; high viral RNA in plasma; massive CD4+ T cell infection.
Phase 2: Steady decline in CD4+ T cells; persistent infections (e.g., Candida albicans), fevers, diarrhea, shingles.
Phase 3 (AIDS): CD4+ T cell count drops below 200/μL; immune system fails; AIDS indicator conditions develop.
Diseases Associated with AIDS
Pathogen/Disease | Disease Description |
|---|---|
Protozoa: Cryptosporidium hominis, Toxoplasma gondii, Cystoisospora belli | Persistent diarrhea, encephalitis, gastroenteritis |
Viruses: CMV (HHV-5), HSV-2, VZV (HHV-3) | Fever, encephalitis, blindness, vesicles, shingles |
Bacteria: Mycobacterium tuberculosis, M. avium | Tuberculosis, disseminated infections |
Fungi: Pneumocystis jirovecii, Histoplasma capsulatum, Cryptococcus neoformans, Candida albicans | Pneumonia, disseminated infections, oral/vaginal overgrowth |
Cancers: Kaposi’s sarcoma, hairy leukoplakia, cervical dysplasia | Cancer of skin/blood vessels, precancerous mucosal patches, abnormal cervical growth |
HIV Diagnosis and Transmission
Diagnosis: Antibody tests (may take up to 3 months for seroconversion), confirmed by Western blot. NAATs detect HIV RNA earlier (10–15 days post-exposure).
Transmission: Blood, semen, breast milk, transplacental, contaminated needles, organ transplants, artificial insemination, blood transfusion. Anal-receptive intercourse is highest risk.
Global HIV/AIDS Statistics
~40.8 million people living with HIV worldwide (2024–2025).
~1.3 million new infections, ~630,000 AIDS-related deaths annually.
Sub-Saharan Africa bears the highest burden (64% of cases).
Prevention and Treatment of AIDS
Biomedical interventions: Condoms, HIV testing, needle programs.
Behavioral interventions: Sex education, counseling.
Structural interventions: Social, economic, and political changes.
Antiretroviral Therapy (ART): Combination of drugs to minimize resistance. Includes pre-exposure (PrEP) and post-exposure prophylaxis (PEP).
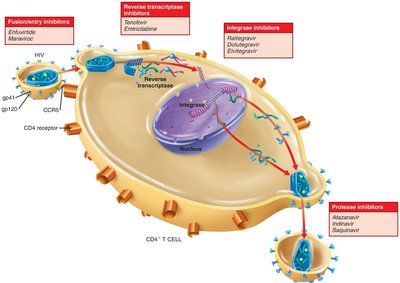
Drug classes:
Cell entry inhibitors (e.g., enfuvirtide, maraviroc)
Reverse transcriptase inhibitors (nucleoside and non-nucleoside)
Integrase inhibitors (e.g., raltegravir, dolutegravir, elvitegravir)
Protease inhibitors (e.g., atazanavir, indinavir, saquinavir)
Maturation inhibitors and tetherins
