 Back
BackMicrobial Diseases of the Urinary and Reproductive Systems
Study Guide - Smart Notes
 Tailored notes based on your materials, expanded with key definitions, examples, and context.
Tailored notes based on your materials, expanded with key definitions, examples, and context.
Microbial Diseases of the Urinary and Reproductive Systems
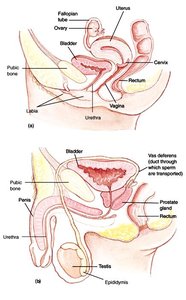
Normal Microbiota of the Urinary and Reproductive Systems
The urinary and reproductive systems have distinct microbiota that play a role in health and disease. The upper urinary tract and bladder are typically sterile, while the lower regions may harbor normal flora influenced by factors such as hormones and anatomical differences.
Urinary bladder and upper urinary tract: Normally sterile in healthy individuals.
Female reproductive tract: Vaginal microbiota is dominated by Lactobacilli during reproductive years, influenced by estrogen levels.
Male urethra: Generally sterile except for the distal end.
Indicators of infection: More than 1,000 bacteria/ml or 100 coliforms/ml in urine suggests infection.
Cystitis (Urinary Bladder Infection)
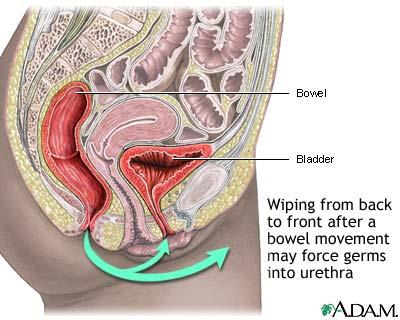
Cystitis is a common infection of the urinary bladder, especially in females, due to anatomical and behavioral factors. It can lead to more severe infections if untreated.
Contributing factors: Microorganisms at the urethral opening, poor hygiene, and sexual intercourse.
Common causative agents: Escherichia coli (most common), Proteus, Klebsiella, Enterococcus, Pseudomonas.
Diagnosis: Antibiotic-sensitivity tests may be required before treatment.
Nosocomial cases: Often associated with catheterization in hospitals.
Complications: Infection can ascend to the kidneys, causing ureteritis and pyelonephritis (75% caused by E. coli).
Sexually Transmitted Diseases/Infections (STDs/STIs)
STDs are a major public health concern, with millions of new cases annually. They can be caused by bacteria, viruses, or parasites and often have significant health and economic impacts.
Prevalence: Over 15 million new cases each year in the US.
Types: More than 30 different STIs, including bacterial, viral, and parasitic infections.
Prevention: Highly effective prevention includes safe sexual practices, regular screening, and vaccination where available.
Bacterial STIs
Gonorrhea
Gonorrhea is a common bacterial STI caused by Neisseria gonorrhoeae. It primarily affects mucosal surfaces and can lead to severe complications if untreated.
Pathogen: N. gonorrhoeae (Gram-negative diplococcus).
Transmission: Attaches to mucosal cells of the oral-pharyngeal area, genitals, eyes, and rectum via fimbriae.
Symptoms in males: Painful urination and pus discharge; complications include urethral blockage and sterility.
Symptoms in females: Often asymptomatic unless infection spreads, leading to pelvic inflammatory disease (PID).
Complications: Endocarditis, meningitis, arthritis, ophthalmia neonatorum in newborns.
Diagnosis: ELISA or PCR tests.
Antibiotic resistance: Increasing due to R-plasmids.
Immunity: No lasting immunity or vaccine available.

Pelvic Inflammatory Disease (PID)
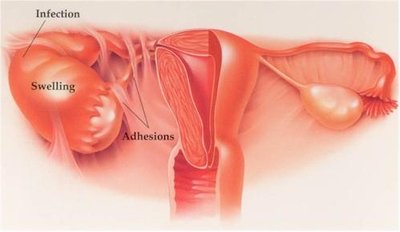
PID is a serious complication of untreated STIs, especially gonorrhea and chlamydia, leading to inflammation and damage of the female reproductive organs.
Causes: Often results from ascending infections by N. gonorrhoeae or Chlamydia trachomatis.
Symptoms: May include abdominal pain, fever, and abnormal discharge; 50% of females may be asymptomatic.
Complications: Tubal infection, salpingitis, scar tissue, adhesions, ectopic pregnancies, sterility, and chronic abdominal pain.
Nongonococcal Urethritis (NGU) – Chlamydia
NGU is most commonly caused by Chlamydia trachomatis, an obligate intracellular bacterium. It is the most frequently reported STI in the US and is often asymptomatic.
Symptoms: 50% of males and 75% of females are asymptomatic; can lead to PID in women.
Complications: Chlamydial ophthalmia and pneumonia in newborns.
Diagnosis: Detection of chlamydial DNA in urine.
Screening: Annual tests recommended for sexually active women under 25 years old.
Syphilis
Syphilis is a chronic STI caused by the spirochete Treponema pallidum. It progresses through several stages and can cause severe systemic complications if untreated.
Pathogen: T. pallidum (spirochete); cannot be cultured in vitro.
Transmission: Direct contact; can invade intact mucous membranes or penetrate skin breaks.
Stages:
Primary: Hard, painless chancre at infection site.
Secondary: Flu-like symptoms, widespread rash; lesions are highly infectious.
Latent: Asymptomatic, may last for years.
Tertiary: Gummas (soft, tumor-like growths), neurosyphilis, cardiovascular syphilis, aortic aneurysms.
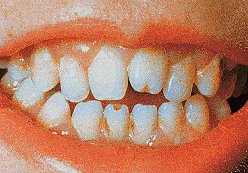
Congenital syphilis: T. pallidum crosses placenta, causing Hutchinson's triad: notched incisors, keratitis, and deafness.
Diagnosis: Darkfield microscopy and serological assays (cannot be cultured).
Treatment: Effective at all stages, but damage is irreversible if already present.
Viral STIs
Genital Herpes
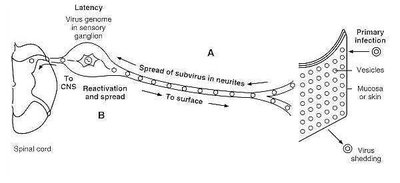
Genital herpes is caused by herpes simplex viruses (HSV-1 and HSV-2). It is a lifelong infection with periods of latency and reactivation.
Prevalence: About 16.2% of people aged 14–49 in the US have genital HSV-2 infection.
Symptoms: Painful urination, genital irritation, fluid-filled vesicles.
Neonatal herpes: Can cause neurological damage or death if contracted during birth.
Latency: Virus remains dormant in nerve cells; recurrences triggered by trauma, stress, or hormonal changes.
Transmission: Highly transmissible, even during asymptomatic shedding.
Treatment: Suppressive therapy with acyclovir and related drugs.
Genital Warts
Genital warts are caused by human papillomaviruses (HPV), with certain strains linked to cancer. Vaccination and screening are important preventive measures.
Prevalence: About 20 million Americans currently infected; 6 million new cases annually.
High-risk strains: HPV 16 and 18 associated with cervical and penile cancer.
Diagnosis: DNA testing for cancer-causing strains; importance of Pap smear screening.
Prevention: Vaccines (Gardasil, Cervarix) recommended for boys and girls aged 9–26 years.
Parasitic STIs
Trichomoniasis
Trichomoniasis is a common, curable STI caused by the protozoan Trichomonas vaginalis. It often presents with symptoms in women but is usually asymptomatic in men.
Prevalence: 7.4 million new cases per year in the US.
Symptoms in women: Frothy, yellow-green vaginal discharge with a strong odor.
Symptoms in men: Usually asymptomatic; men serve as reservoirs.
Diagnosis: Observation of motile protozoa in wet mounts from infection site.
Treatment: Metronidazole is effective.
